


Daniel Holanda Barroso1; Clarrissa Marques Maranhão1; Araken Almeira de Araújo2; Eliane Ruth Barbosa Alencar3; Emmanuel Rodrigues de França4; Silvana Maria de Morais Cavalcanti2
Erythroplasia of Queyrat is an in situ squamous cell carcinoma of the glans penis. Due to its unusual location, surgical treatment can cause mutilation. CO2 laser-assisted vaporization is a treatment option with excellent aesthetic and functional results, but it requires strict follow up owing to its high recurrence rates. The authors describe a case of erythroplasia of Queyrat treated with fractional CO2 laser, with an absence of recurrence during a one-year follow up
Keywords: CARCINOMA, SQUAMOUS CELL; CARCINOMA IN SITU; FORESKIN; LASER COAGULATION; LASERS; LASERS; GAS; PENIS; PENILE NEOPLASMS
The traditional treatment for squamous cell carcinoma of the penis is resection with a 2 cm safety margin. 1 This procedure, however, is considered mutilating, and conservative treatments are accepted for in situ lesions.2 Treatments with imiquimod, 5-fluorouracil, and laser are described in the literature. 2
CO2 laser is absorbed by water and produces deep, predictable cutaneous vaporizing regardless of the color of the tissue.3 The authors report a case of a patient with erythroplasia of Queyrat treated with CO2 fractional laser.
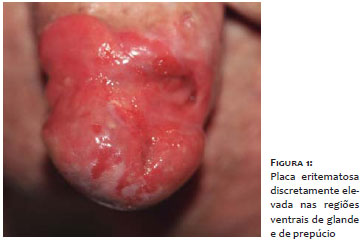
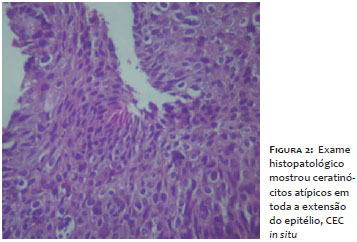
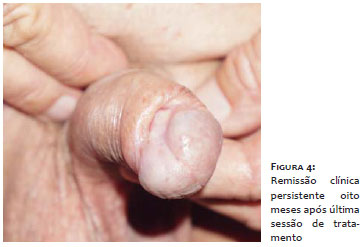
An 80-year-old man with hypospadias complained of a reddish lesion, progressive in growth that had appeared in the periurethral region one year earlier. On examination it was possible to observe an erythematous plaque in the ventral portions of the glans and foreskin (Figure 1). Biopsies were performed on four specimens, each obtained from one of four quadrants of the lesion, in addition to the exeresis of its most elevated part. The histological examination revealed a squamous cell carcinoma (SCC) in situ: erythroplasia of Queyrat (Figure 2). The patient refused to undergo excision of the lesion, preferring the treatment with CO2 fractional laser (eCO2®, Lutronic, Sowon-Ro, South Korea). The procedure was performed monthly under topical anesthesia with 4% lidocaine cream (Dermomax®, Laboratório Aché, São Paulo, Brazil). During each procedure the coagulation of all the spongy area was carried out with a 5 mm margin. The parameters used were: 300µµ tip, 100mtz/cm2 density, and 60 to 80J/cm2 fluence. Five sessions were performed (Figures 3 and 4). There were no complications between sessions. By the time this paper was approved for publication, the patient had not presented recurrences for a period of one year and would be followed up with for five years after the end of the treatment.
The erythroplasia of Queyrat (EQ) is an SCC in situ that develops in the glans or foreskin. 4 Its extension up to the distal urethra - where the pseudostratified urethral epithelium becomes squamous stratified - has already been described. 5 The EQ usually arises in the glans and inner foreskin as a single plaque or multiple plaques that are slightly elevated and erythematous.4 When compared to SCC in situ of the epidermis, the EQ has a high rate of progression into invasive neoplasia (10-33%).4,6
Conventional treatment of penile carcinoma involves full or partial amputation with good oncologic control of the lesion,7 however aesthetic and functional alterations may affect psychosexual function in important ways. Conservative therapy is an option for in situ lesions,2 and although survival is seldom affected, it has a higher recurrence rate when compared to the surgical treatment described.7
Mohs micrographic surgery is a conservative treatment option, however it has a relatively high recurrence rate (21%) when compared to partial penectomy (0-7%).8 Due to the extent of the lesion, even undergoing Mohs micrographic surgery would be unacceptable to the patient because of the great loss of tissue.
Of the topical alternatives, 5-fluorouracil is the most studied,4,2 even though it causes great discomfort and a local inflammatory process during different treatment cycles.4 When the urethra is affected, however, this treatment is not recommended by some authors,4 since there is no guarantee that it will be possible to perform applications along the entire length of the intraurethral lesion.9
According to the last U.S. directive,2 CO2 or ND:YAG laser therapy are among the options for penile SCC in situ, and some consider this as the first choice due to the favorable aesthetic and functional outcomes.1 On the other hand, local recurrence rates are high, reaching 26%; 1 therefore, patients should be followed up with more often than those who underwent amputation - every three months for the first two years and every six months up until five years after the treatment.6 Recurrences can be treated with the same procedure.1
Nd:YAG laser produces tissular coagulation at least 3-4mm1 deep, a very useful benefit in cases of histologically aggressive and invasive tumors.10 On the other hand, it tends to result in unsightly scars.1 In contrast, CO2 laser is absorbed by water and has a superficial vaporization effect with predictable depth (0.1 - 0.23 mm),3 and is considered the best laser for the treatment of non-invasive lesions. 1 Its use was reported in the involvement of the proximal urethra, with good results. 5 In these cases, the possibility of stenosis 5 and intraurethral recurrence of the lesion requires a multidisciplinary approach with urology.
Another peculiarity of the case is the association with hypospadias. A search on the PubMed database with the keywords Queyrat, hypospadia, carcinoma and penis yielded only one case report of association between hypospadias and penile SCC.1
1. van Bezooijen BP, Horenblas S, Meinhardt W, Newling DW. Laser therapy for carcinoma in situ of the penis. J Urol. 2001;166(5):1670-1.
2. Clark PE, Spiess PE, Agarwal N, Biagioli MC, Eisenberger MA, Greenberg RE, et al. Penile cancer: Clinical Practice Guidelines in Oncology. J Natl Compr Canc Netw. 2013;11(5):594-615.
3. Shokrollahi K, Raymond E, Murison MSC. Lasers: principles and surgical applications. The Journal of Surgery. 2004;2(1):28-34.
4. Graham JH, Helwig EB. Erythroplasia of Queyrat. A clinicopathologic and histochemical study. Cancer. 1973;32(6):1396-414.
5. Del Losada JP, Ferré A, San Román B, Vieira V, Fonseca E. Erythroplasia of Queyrat with urethral involvement: treatment with carbon dioxide laser vaporization. Dermatol Surg. 2005;31(11 Pt 1):1454-7.
6. Mikhail GR. Cancers, precancers, and pseudocancers on the male genitalia. A review of clinical appearances, histopathology, and management. J Dermatol Surg Oncol. 1980;6(12):1027-35.
7. Leijte JA, Kirrander P, Antonini N, Windahl T, Horenblas S. Recurrence patterns of squamous cell carcinoma of the penis: recommendations for follow-up based on a two-centre analysis of 700 patients. Eur Urol. 2008;54(1):161-8.
8. Shindel AW, Mann MW, Lev RY, Sengelmann R, Petersen J, Hruza GJ, et al. Mohs micrographic surgery for penile cancer: management and long-term followup. J Urol. 2007;178(5):1980-5.
9. Bernstein G, Forgaard DM, Miller JE. Carcinoma in situ of the glans penis and distal urethra. J Dermatol Surg Oncol. 1986;12(5):450-5.
10. Frimberger D, Hungerhuber E, Zaak D, Waidelich R, Hofstetter A, Schneede P. Penile carcinoma. Is Nd:YAG laser therapy radical enough? J Urol. 2002;168(6):2418-21.
This study was carried out at the Universidade de Pernambuco - Recife (PE), Brazil.
 All content the journal, except where identified, is under a Creative Commons Attribution-NonCommercial 4.0 International license - ISSN-e 1984-8773
All content the journal, except where identified, is under a Creative Commons Attribution-NonCommercial 4.0 International license - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}