


Kássila da Rosa Nasser1; Luiz Carlos Cuce2; Rossana de Farias Vasconcelos3; Ana Carolina Macedo4; Juliana Garcia Kako Rodriguez5; Rodrigo Garcia Arruda6; João Guilherme Finizola7
Case report of a male patient bearing a rare granular cell tumor in the left arm, confirmed by histology and immunohistochemistry (positive S100 and CD68 proteins).
Keywords: ARM; GRANULAR CELL TUMOR; SKIN NEOPLASMS
The granular cell tumor (GCT), originally known as the Abrikossof tumor, is rare and of unknown origin. 1
Formed by cells with granular cytoplasm, it has benign features, and cases of malignancy are rare. It is slightly more frequent in women and people of African origin, and mainly occurs within the third to the fifth decade of life.1-3
It is clinically characterized as a solitary, asymptomatic nodule, usually located in the head and neck (45-65%). Of these, 70% are located in the oral cavity (tongue and oral mucosa), although there are reports of its presence in other organs.4
The diagnosis is performed with histological and immunohistochemical examinations. It has a typical histology that shows a poorly defined, non-encapsulated nodule with polygonal cells, abundant granular cytoplasm, with small round nuclei and prominent nucleoli. Its cells are strongly S-100 positive in the immunohistochemical tests.
The authors describe a case of this tumor having a rare location, not previously described in the literature.
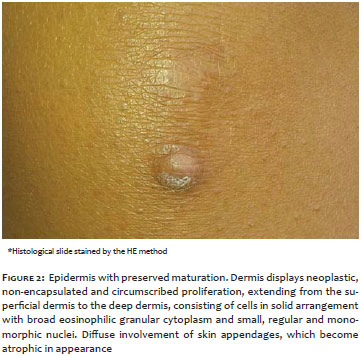
A 30-year-old male patient attended a consultation for an asymptomatic nodular cystic lesion in the left arm measuring 1.3 x 0.8 cm that had been developing for two years. (Figure 1).
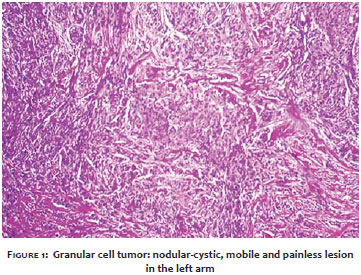
An excisional biopsy of the lesion was carried out, with the histological study suggesting an absence of alterations in the epidermis and dermis with non-encapsulated and circumscribed neoplastic proliferations up to the deep dermis, consisting of cells in a solid arrangement, with broad granular eosinophilic cytoplasm and small, regular monomorphic nuclei. The skin appendages were atrophic (Figure 2).
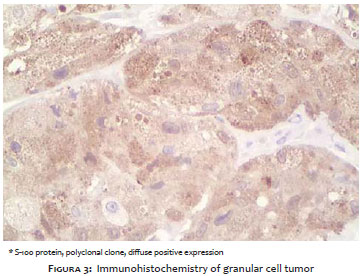
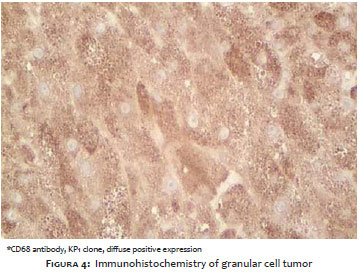
The S-100 (Figure 3) and CD68 (Figure 4) proteins were dimly positive in the immunohistochemical test - clone KP1. The other proteins - such as p53, Melan-A, HMB45, desmin, CK5, CD34, AML, AE1+AE3 came out negative, invalidating the hypothesis of melanocytic epithelial, muscular, or vascular neoplasia.
There are scarce reports of GCT in the literature. Typical locations for the tumor are the head and neck, with the oral mucosa being the most common. In the literature there were no reports of the tumor being present in the upper limbs, as in the case described in this paper.
Its origin is still unknown. In the past it was believed that this cell type originated in the smooth muscles, however some studies assume it arises from the nerve sheath cells - the Schwann cells - in which there is positivity for the S-100 protein. 5
In recent years, immunohistochemical markers that are positive for GCT, with positive immunoreactivity for alpha-1-antitrypsin and CD68 have been developed. CD68 is closely linked to the lysosomal membrane glycoprotein. The positive immunoreactivity for alpha-1-antitrypsin and CD68 in GCT may reflect the intracytoplasmic accumulation of phagolysosomes and does not imply histiocytic origin for these tumors.5,6 From a practical point of view, therefore, only S-100 staining could be used to confirm the diagnosis.
Tumor treatment is performed through surgical resection within adequate margins, with the material being sent to histologic examination, as done in the present case. On rare occurrences of multiple tumors, intralesional injection of glucocorticoids can be carried out with an aim at temporarily reducing the size of the lesions, with spontaneous regression occurring in some cases. 7
The malignancy of the tumor is controversial, since there have already been reported cases of malignant GCT. Its malignant variant can metastasize, and is more common in children and in the gingival region.
In face of this tumor's atypical and not yet published location, in addition to the scarcity of reported cases, the authors emphasize the necessity of further studies aimed at deepening the knowledge on the subject. The authors also highlight the importance of surgical resection as it can possibly be a malignant lesion.
1. Brandão M, Domenech J, Noya M, Sampaio C, Almeida MVC, Guimarães NS, et al. Tumor de células granulares no pé (tumor de Abrikossoff): localização infreqüente de tumor relativamente raro. An Bras Dermatol. 2001;76(2):215-22.
2. Calonje E. Soft-Tissue Tumours and Tumour-like Conditions. In: Burns T, Breathnach S, Cox N, Griffiths C, eds. Rook’s Textbook of Dermatology. 8th ed. Oxford: Wiley-Blackwell; 2010. p. 56.50.
3. Zangari F, Trombelli L, Calura G. Granular cell myoblastoma. Review of the literature and report of a case. Minerva Stomatol. 1996;45(5):231.
4. Ortiz-Hidalgo C, de la Vega G, Moreno-Collado C. Granular cell tumor (Abrikossoff tumor) of the clitoris. Int J Dermatol. 1997;36(12):926-37.
5. Filie AC, Lage JM, Azumi N. Immunoreactivity of S100 protein, alpha-1-antitrypsin, and CD68 in adult and congenital granular cell tumors. Mod Pathol. 1996;9(9):888-92.
6. Cavaliere A, Sidoni A, Ferri I, Falini B. Granular cell tumor: an immunohistochemical study. Tumori. 1994;80(3):224-8.
7. Baraf CS, Bender B. Multiple cutaneous granular cell myoblastoma. Arch Dermatol. 1964;89:243-6.
This study was carried out at the Universidade de Santo Amaro - Santo Amaro (SP), Brazil.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}