


Lara Caroline Grander1; Solange Cardoso Maciel Costa Silva2; Alice Paixão Lisboa3; Virginia Pinheiro de Souza4; Fernanda Cabral3
The upper lip is commonly affected by cutaneous carcinomas. The excision of the neoplasia with safe oncologic margins calls for a large incision, and sometimes flaps are necessary. In addition to its aesthetic value, a successful lip reconstruction includes the maintenance of perfect oral functionality. The authors describe a nasolabial rotation cutaneous flap associated with an advancement flap of the oral mucosa in a single surgical event, performed on a patient bearing basal cell carcinoma involving the left side portion of the upper lip.
Keywords: SURGICAL FLAPS; CARCINOMA, BASAL CELL; MOUTH MUCOSA
Lip carcinomas account for approximately 25% of all oral tumors.1 Late diagnosis and the need for safety margins often result in the primary defect covering a quarter to one third of the upper lip, thus preventing direct suture.2 The reconstruction of defects in the upper lip has been shown to be a surgical challenge. There is no specific method to be used for lesions in the lateral area of the upper lip.
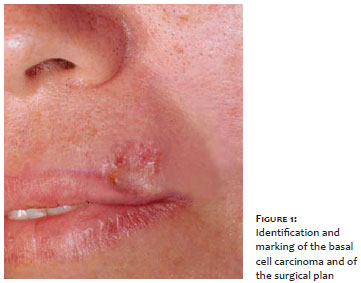
The present paper reports the case of a 48-year-old female patient bearing for the span of one year an erythematous plaque, 2 cm in diameter, having pearly borders and well-defined contours in the lateral third of the upper lip. Ovoid nests and arboriform vessels were evidenced by dermoscopy. The invasive micronodular basal cell carcinoma diagnosis was confirmed by an incisional biopsy. In the absence of lymphadenopathy and any signs and symptoms, the lesion was classified as Stage I (T1N0M0).3
Due to the essential need for a complete exeresis of the tumor, combined with the preparation of a local flap, the excision and surgical reconstruction were carried out in one single event. The objective of the present report is to describe the reconstruction technique and demonstrate its surgical applicability, as well as its aesthetic and functional outcomes.
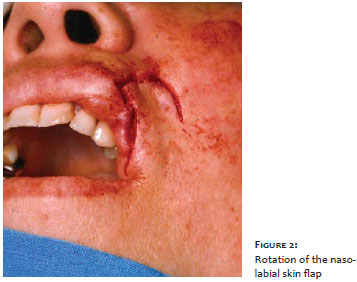
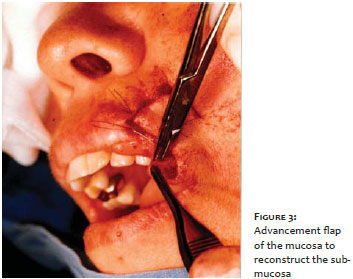
The tumor was identified and underwent resection with a 5 mm surgical margin (Figure 1). A rotation flap in the nasolabial fold was used to fill the open area of skin in the upper lip (Figure 2). The reconstruction of the submucosa was performed with an advancement flap of the buccal mucosa (Figure 3). Finally, the suture of the primary and secondary defects was carried out.
The histologic examination of the removed specimen confirmed the presence of margins free of neoplastic involvement. The patient developed post-surgical stress labial herpes, but showed good response to treatment with oral acyclovir in a weekly follow up during the first month. Figure 4 shows the two-week outcome after the surgery.
The single-stage procedure, combining an upper lip reconstruction after excision of basal cell carcinoma, was performed on the patient using a nasolabial rotation flap associated with an advancement flap of the buccal mucosa, with margins free of neoplastic involvement and an excellent aesthetic appearance.
The reconstruction of the upper lip has consistently been a challenge for surgeons, since the contour, symmetry and cupid's bow positioning of the lip must be kept unchanged,4,5 and the functionality of the mouth opening preserved as well.1,4
For minor lesions, "V" and "W"-shaped excisions followed by suturing are sufficient.5,6 However, when lesions extend from one to two thirds of the lip, local flaps are the best choice - such as 2 i) the Abbé,6 ii) the Estlander,2,6,7 iii) the Gillies unilateral,5 iv) the Karapandzic unilateral,5 and v) the "V-Y"-shaped. 8
Primary defects affecting 80% or more of the lip can be reconstructed with i) bilateral Karapandzic and Gillies flaps, 5,6 ii) Fujimori flap, 9 iii) Bernard von Burrow Webster technique, 2,6,10 and iv) antebrachial microsurgical flap.2
In the present example, a primary suture was contraindicated due to the displacement it would cause to the philtrum and the general asymmetry that would result. The Abbé flap would be a plausible option for the case, however it would have disadvantages such as scar formation in the lower lip, the inconvenience of having to be performed in two stages, in addition to the patient's discomfort of not being able to open the mouth in the first 14 to 21 days post-operatively. 5
Comparing the technique used in this example with the flaps described to date in the literature, it is possible to conclude that the aesthetic and functional outcomes provided to the patient were excellent. The practical demonstration of the nasolabial and submucosal flap, carried out in a single surgical procedure, allowed for an absence of tension, reconstruction of the skin and submucosa without distortion of the upper lip, a minimal surgical scar hidden in the nasogenian fold and the maintenance of the oral function in a young adult patient.
1. Vaienti L, Zilio D, Di Matteo A, Riccio M, Marchesi A. Central upper lip reconstruction by two vermillion flaps and a rotational skin flap. Dermatology. 2012;224(2):130-3.
2. Anvar BA, Evans BCD, Evans GRD. Lip reconstruction. Plast Reconstr Surg. 2007;120(4):57e-64e.
3. Dourmishev L, Rusinova D, Botev I. Clinical variants, stages, and management of basal cell carcinoma. (Review Article). Indian Dermatol Online J. 2013;4(1):12.
4. Lopes Filho LL, Soares Lopes LR, De Barros Villa Neto A, De Sousa Costa T. Carcinoma basocelular no lábio superior: tratamento cirúrgico e reconstrução com retalho de transposição. Surg Cosmet Dermatol. 2011;3(3):243-5.
5. Neligan PC. Strategies in Lip Reconstruction. Clin Plast Surg. 2009;36(3):477-85.
6. Contin LA, de Carvalho MM, Filho CDSM, Hayashida ME, Ferraz TS, Gonçalves Jr. BF. Reconstrução do lábio inferior com retalhos de Karapandzic e Gilles após excisão de carcinoma espinocelular. Surg Cosmet Dermatol. 2012;4(1):195-9.
7. Genc S, Ugur SS, Arslan IB, Tuhanioglu B, Demir A, Selcuk A. Lower lip reconstruction with Abbe-Estlander flap modification: preserving the same side vascular pedicle. Eur Arch Otorhinolaryngol. 2012;269(12):2593-4.
8. Narsete TA. V-Y advancement flap in upper-lip reconstruction. Plast Reconstr Surg. 2000;105(7):2464-6.
9. 9. Aytekin A, Aytekin O. Total upper lip reconstruction with bilateral Fujimori gate flaps. Plast Reconstr Surg. 2003;111(2):797-800.
10. 10. Seo HJ, Bae SH, Nam SB, Choi SJ, Kim JH, Lee JW, et al. Lower lip reconstruction after wide excision of a malignancy with barrel-shaped excision or the Webster modification of the Bernard operation. Arch Plast Surg. 2013;40(1):36-43.
This study was carried out at the Universidade Estadual do Rio de Janeiro (UERJ) - Rio de Janeiro (RJ), Brazil.
 All content the journal, except where identified, is under a Creative Commons Attribution-NonCommercial 4.0 International license - ISSN-e 1984-8773
All content the journal, except where identified, is under a Creative Commons Attribution-NonCommercial 4.0 International license - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}