


Breno Augusto Campos de Castro1; Juliana Cristina Silva Fraga2; Moisés Salgado Pedrosa3; Dalila Raquel de Almeida Marques2; Viviane Priscila Gonçalves2; Juliana Milagres Macedo Pereira1
A Wood's lamp is a cost effective, safe, easy to use diagnostic tool that is readily available at medical practices. However, its dermatological application has been restricted to the detection of cutaneous infections, the evaluation and classification of pigmentation disorders (such as melasma and vitiligo), and the analysis of disturbances in the metabolism of porphyrins. In the present report the authors demonstrate the use of a Wood's lamp as an alternative to confocal optical microscopy, in the delimitation of the surgical margins of a hypomelanotic lentigo maligna melanoma, whose lack of melanin pigmentation and tumor location in a photodamaged area had hampered a patient's surgical planning.
Keywords: LIGHT; MELANOMA; MELANOMA, AMELANOTIC; MICROSCOPY, CONFOCAL;
The Wood's light (WL) has been used by dermatologists as a diagnostic device in pigmentary disorders, skin infections, and porphyria for more than a century. 1 Although it is an easy to use and cost effective tool, it is also often an underutilized tool. Very few publications explore its new applications. Paraskevas et al. 2 demonstrated its use in the detection of recurring pigmentation in surgical scars, in the differentiation between agminated nevus and spilus nevus, and the in the delimitation of surgical margins in lentigo maligna.
The present paper describes a case of hypomelanotic lentigo maligna melanoma, where visual inspection and dermoscopy were insufficient to define the lesion's surgical borders.
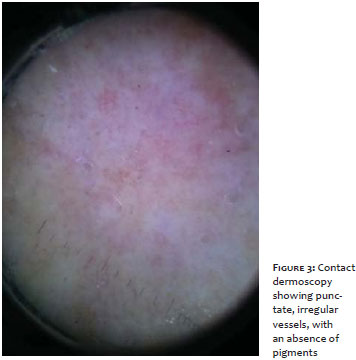
A seventy-four year-old female patient, Fitzpatrick skin phototype II, with a history of multiple basal cell carcinomas, complained of an erythematous lesion that she had noticed in the right infraclavicular region ten months earlier. Dermatological examination showed a 4.2 cm x 3.1 cm erythematous-brownish macule with irregular and poorly defined borders (Figures 1 and 2). Dermoscopy evidenced a lesion with an erythematous background, without evident pigmentation, and rare punctate, irregular vessels that intermingled with areas of photodamage (Figure 3). After a clinical evaluation, an incisional biopsy was carried out with the histological study of the sample suggesting the diagnosis of hypomelanotic lentigo maligna melanoma (HLMM) in a radial growth phase, with a thickness of 0.25 mm.
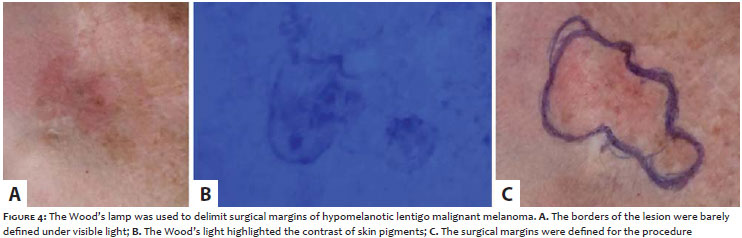
The WL was used in the pre-operative evaluation in order to delimit the surgical margins of the HLMM (Figure 4A). The patient then underwent tumor exeresis and a primary closure (Figure 4B). The authors decided to carry out the resection with a 1 cm margin due to the possibility of performing the primary closure as well as concerns about the loss of the case follow-up. The histology revealed the proliferation of atypical epithelioid melanocytes, and voluminous, hyperchromatic, pleomorphic nuclei with evident nucleoli, in addition to lentiginous distribution in the dermoepidermal junction. It was also possible to notice the absence of ulceration or mitotic figures, a Breslow index of 0.32 mm, Clark level III and free margins (Figure 4C). The patient is currently being followed up at the Dermatology Service, without signs of recurrence.
The WL is an observation and diagnosis tool based on the fluorescence phenomenon of the cutaneous surface. 1 The long wave ultraviolet radiation (UVR) emitted by the WL originates from a high-pressure mercury arc passing through a barium silicate filter containing 9% of nickel oxide, called Wood filter. 1 This filter allows the passage of UVR waves that are in the range 320nm - 400nm, with a peak at 365nm. Melanin is responsible for the absorption of most of the radiation emitted by the WL. In cases of skin lesions with an increased concentration of epidermal melanin, the dermatologist will see it in darker contrast to the circumscribed normal skin. In cases of a lower concentration of melanin, lesions will tend to be lighter and more difficult to distinguish.1,2
In the evaluation of lesions with poor melanin pigmentation or in regions of extensive photodamage, examination under visible light is often insufficient to distinguish areas of fair pigmentation from normal skin areas, due to lack of contrast. This is mainly due to the fact that the longer wavelengths of light present in the visible light spectrum penetrate deeper into the dermis than the shorter wavelengths. The dermis reflects longer wavelengths and thus reduces the contrast of the image that is perceptible to the examiner's eye. When only shorter wavelengths of WL are used to illuminate the skin, the interference caused by the longer wavelengths is avoided, consequently improving the contrast between superficial pigmented lesions and the normal epidermis.2
Due to this ability to emphasize the different pigmentation of the skin, WL becomes a tool of considerable value in the pre-operative evaluation of hypomelanotic tumors or tumors located in areas of extensive sun damage. Although most melanomas are characterized by a pigmentation that ranges between shades of brown and black, there are numerous reports in the literature of amelanotic malignant melanoma (AMM), which is characterized by the complete absence of pigment, or more frequently, with melanin pigmentation in less than 25% of the total lesion area, called hypomelanotic malignant melanoma (HMM).3, 4
AMMs correspond to a range of 1 - 8% of melanomas. Any cutaneous melanoma subtype can be amelanotic, although the subungual and desmoplastic variants have the highest rates (15% to 20% and 50%, respectively). 5 Therefore, the amelanotic or hypomelanotic lentigo malignant melanoma is rare, constituting a diagnostic challenge, especially when the dermatologist needs to define its borders for surgery. Although laser assisted confocal microscopy 6 is the most accurate technique for the pre-operative study, its high cost and limited availability in most dermatology services in Brazil make WL by contrast an indispensable tool for dermatologists.
1. Asawanonda P, Taylor CR. Wood’s light in dermatology. Int J Dermatol. 1999;38(11):801-7.
2. Paraskevas LR, Halpern AC, Marghoob AA. Utility of the Wood’s light: five cases from a pigmented lesion clinic. Br J Dermatol. 2005;152(5):1039-44.
3. Pizzichetta MA, Talamini R, Stanganelli I, Puddu P, Bono R, Argenziano G, et al. Amelanotic/hypomelanotic melanoma: clinical and dermoscopic features. Br J Dermatol. 2004;150(6):1117-24.
4. Steglich RB, Meotti CD, Ferreira MS, Lovatto L, de Carvalho AV, de Castro CG. et al. Dermoscopic clues in the diagnosis of amelanotic and hypomelanotic malignant melanoma. An Bras Dermatol. 2012;87(6):920-3.
5. Lapresta A, García-Almagro D, Sejas AG. Amelanotic lentigo maligna managed with topical imiquimod. J Dermatol. 2012;39(5):503-5.
6. Mofarrah R, Ahigrimm-Siess V, Massone C, Hofmann-Wellenhof R. Reflectance confocal microscopy:a useful and non-invasive tool in the in vivo differentiation of benign pigmented skin lesions from malignant melanoma. Reporto f a case. Dermatol Pract Concept. 2013;3(1):33-5.
This study was carried out at the Hospital of the Hospital da Polícia Militar de Minas Gerais - Belo Horizonte (MG), Brazil.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}