


Eloisa Leis Ayres1; Paula Ferrazzi Magrin2; Fabíola Bentivoglio3; Adilson Costa4
Introduction: Progressive macular hypomelanosis is characterized by the emergence of hypopigmentation, predominantly in the trunk region of young women of mixed racial origin. Although recent studies suggest that Propionibacterium acnes may have an important role in the pathogenesis, its etiology remains unclear. Objective: To evaluate the prevalence of the condition with regards to gender, age, skin phototype, affected areas and disease onset, and the relationship with ordinary acne and oily skin in the city of Niterói, Rio de Janeiro State, in the coastal region of Southeast Brazil. Methods: Retrospective epidemiological study that uses the analysis of medical records of 103 patients with diagnosis of progressive macular hypomelanosis, from 2001 to 2012. Results: Eighty-two percent of studied patients were women and 18% men, with a predominance of phototypes III (42.7%) and IV (42.7%). The average age of onset of the disease at diagnosis was 26 years. In 46.0% of patients the disease duration ranged from 1 to 4 years. When two areas were affected (50%), the dorsum was the most frequent (79.0%), followed by the abdomen (20.0%). In 98% of cases, patients had oily skin, and 71.8% had active acne. Conclusion: Progressive macular hypomelanosis is a chronic condition that primarily affects the skin of the dorsum and abdomen of young women with skin phototypes III and IV, who are also bearers of oily skin and acne. There are still many doubts regarding the true etiology and treatment of progressive macular hypomelanosis. The high percentage of association with skin oiliness and acne vulgaris suggests that these clinical conditions are possibly related.
Keywords: HYOPIGMENTATION; EPIDEMIOLOGY; ACNE VULGARIS
Progressive macular hypomelanosis (PMH) is a cutaneous condition characterized by the emergence of hypopigmentation, predominantly in the trunk region of young women of mixed racial origin. It is a common, yet underdiagnosed pigmentary disorder. The condition can be found in patients worldwide, however it is more common in those from tropical and subtropical countries.
This entity was first described in 1987 by Borelli2 as cutis trunci variata and named by Guillet in 1988 as progressive macular hypomelanosis.3 Although this became the preferred terminology, it has been recognized by several authors around the world under a wide variety of denominations, such as: hypomelanose maculeuse confluent et progressive du metis melanoderme,4 creole dyschromia,5 idiopathic macular hypomelanosis of the melanodermic, 5 and progressive trunk hypomelanosis.6
Its etiology remains unknown despite several factors having already been suggested as causes for the lesions: racial origin and, later on, a suggested correlation with tinea versicolor and pityriasis alba.3 The presence of Propionibacterium acnes producing a depigmentation factor has also been proposed, as well as disorders in the melanosomes. 7 Hereditary factors may play an important role, although further investigations are necessary.8
PMH is characterized by hypopigmented macules of undefined limits, usually 10-30 mm in diameter, located predominantly in the trunk region of the body. The condition generally affects skin areas rich in sebaceous glands.9 There is typically no reference to previous inflammatory occurrences or lesions of an infectious nature.
The diagnosis is mostly clinical and can be confirmed by examination using a Wood's lamp, which shows red fluorescent spots. 10 Observation with confocal microscopy shows that the "pigmented ring" around the dermal papillae in the lesions is intact, however its melanin content is less than the that of the surrounding normal skin.10 No spores, hyphae or bacteria are observed in the stratum corneum.8 Histological investigations show a slight reduction of melanin granules in the basal cell layer with a variable reduction of melanin transfer to keratinocytes. Nonetheless, the histological findings are not sufficient to characterize the definitive diagnosis of this condition.11
It is necessary to exclude the possibility of pityriasis versicolor, pityriasis alba, leprosy and hypochromic fungoid mycosis as differential diagnoses.11
Several treatments are mentioned in the literature: topical and oral antibiotics, benzoyl peroxide, and phototherapy (PUVA and UVB-NB) - all of which are unstable and still produce results that are not fully satisfactory.12-15
The present study is aimed at evaluating the prevalence of the dermatosis in regards to gender, age, skin phototype, affected areas and duration of the disease, and also considering its correlation with acne vulgaris and oily skin conditions.
A retrospective study was performed through the analysis of medical records of patients with clinical diagnosis of PMH treated at private dermatology practices in the city of Niterói (Rio de Janeiro State), in the coastal region in southeastern Brazil, between 2001 and 2012. The study included 103 patients with complete personal and epidemiological data, and whose diagnosis was conclusive for this disease.
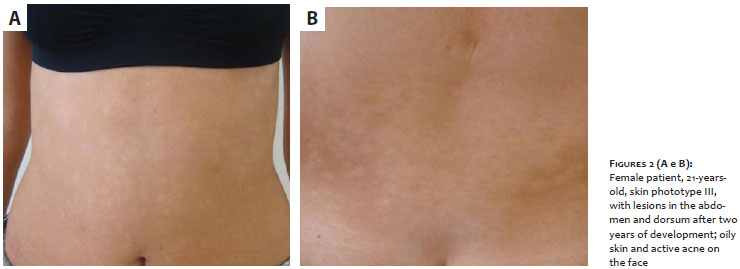
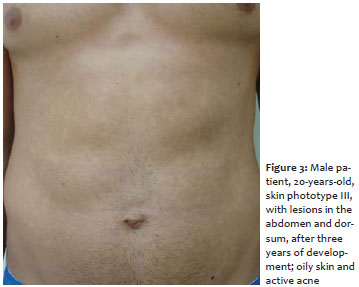
From Table 1 it is possible to note that roughly 82% of the patients were female (Figures 1 and 2), and 18% male (Figures 3 and 4). There was a predominance of phototypes III (42.7%) and IV (42.7%). The patients' mean age at diagnosis was 26 years (min = 13 years, max = 50 years, mode = 22).
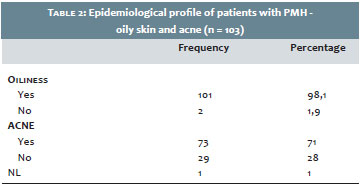
According to Table 2, patients had oily skin in 98% of cases, and 71% had active acne, indicating a possible association of the disease with oily skin and the presence of acne.
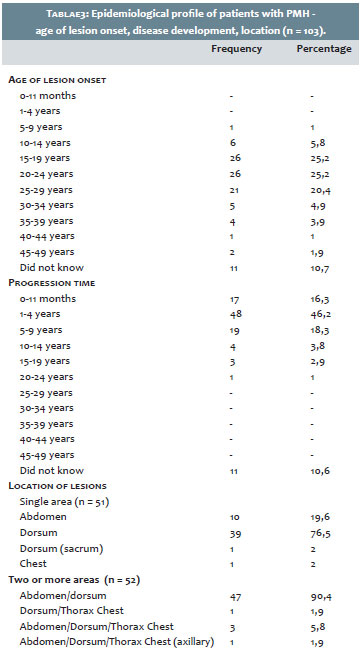
The results in Table 3 indicate that for most evaluated patients, the disease arose between the ages of 15 and 29, with 25% of cases between 15 and 19, 25% between 20 and 24, and 20% between 25 and 29 years. In addition, only 16% had developed the disease less than one year before, and in 46% the time of onset was one to four years before, with 18% with between five to nine years. It is worth noting that some patients had never noticed the lesion or did not exactly know when it had developed, with 4% of patients having more than 15 years of development without remission. One patient reported the development of the picture for about 20 years. Regarding the location, 51 patients had lesions only in one area, and 52 in two or more areas. When the patient had a single lesion, the dorsum was the most often affected area (79%), followed by the abdomen (10 cases, 20%) and chest (one case, 2%). Analyzing the association of affected areas, 47 patients (90%) had concomitant lesions on the dorsum and abdomen, and three patients (6%) had concomitant lesions in the dorsum, abdomen and chest.
Despite the fact that PMH is a considerably common disorder, its true prevalence is unknown.13 It mainly affects young individuals, predominantly between the ages of 18 and 25 years, with rare reports of cases in patients over the age of 50.16 The majority of cases occur in women, in proportions ranging from 3:1 to 7:1,9,13 though some authors have not found differences in the distribution between the genders.2, 17 The present study evaluated 103 patients with clinical diagnosis of PMH. Of these, 82% were female, with 70.8% reporting the lesions' onset at between 15 and 29 years of age, thus corroborating the literature findings. It is important to note that in the present study it was possible to observe cases in men, in all skin phototypes and with onset of lesions between 9 and 49 years old.
Regarding the skin phototype, the literature has divergent data: while some authors found an increased incidence in patients of mixed ethnic origin (Negroids/Caucasoids),12, 13, 18 other studies deny this claim,1, 2, 12 explaining that the disease is probably more easily seen in patients with pigmented skin. Among the present study’s patients, 85.4% had Fitzpatrick phototypes III and IV.
Although some authors incriminate the Propionibacterium acnes as the etiologic agent of this condition, the presence of acne vulgaris associated with HMP was an uncommon finding in some studies. It is also relevant to note that with conventional identification methods, there are still practical difficulties in distinguishing the species or subspecies of some specific genres that can play an important role in the pathogenesis of diseases. In this manner, the Propionibacterium acnes species causing acne and progressive macular hypomelanosis could be of different subtypes.9 In a study by Rodriguez in Spain, of 10 patients with a clinical picture of PMH, seven reported association with acne, however the author himself questions the possibility of different subtypes of this bacteria.19 In the present study, 71% of patients had acne vulgaris as an associated complaint. In addition, oily skin was observed in a significant percentage (98%), in line with studies from other authors.9
Twenty patients had lesions limited to the dorsum; eight had lesions only in the abdomen; 20 had lesions in both the dorsum and abdomen; two had concomitant lesions in the chest in addition to the dorsum and abdomen; and only one had lesions exclusively in the chest. These findings are consistent with the literature, showing the lesions' predominant distribution to be in the dorsal and abdominal regions.
The progression of the lesions is uncertain. Spontaneous regression usually occurs within 3 to 5 years, though some cases persist for more than ten years.4 Menke et al. do not believe in spontaneous remission. On the contrary, they observed stability of the lesions in a 10-year follow up of patients, with no repigmentation being observed in any of them.6 Lesuer et al. showed that lesions may persist for in excess of 25 years.20 In the patients evaluated in the present study, the lesions' time progression at diagnosis ranged from two months to 240 months, with 11 of the 103 patients being unable to specify the exact onset time of the disease due to the fact they had not noticed its presence, and because the lesions were only identified at the dermatological examination.
PMH is a chronic disease that primarily affects the skin of the dorsum and abdomen of young women with phototypes III and IV, oily skin, and acne.
Although several studies have been previously carried out, there are still many doubts regarding PMH, and its true etiology and effective treatment remain under question. The present review reinforces the findings described in the literature, with the high number of patients with skin oiliness and acne vulgaris inducing the authors' belief that the condition's etiology is related to these clinical conditions. Further studies are necessary to confirm the actual involvement of P acnes or subtypes of this bacterium in the etiology of PMH and to further elucidate this disease.
1. Hwang SW, Hong SK, Kim SH, Park JH, Seo JK, Sung HS, et al. Progressive macular hypomelanosis in korean patients: a clinicopathologic study. Ann Dermatol. 2009;21(3):261-7.
2. Borelli D. Cútis trunci variata: nueva genodermatosis. Med Cutan Ibero-Lat-Am. 1987;15:317-319.
3. Guillet G, Helenon R, Gauthier Y, Surleve-Bazeille JE, Plantin P, Sassolas B. Progressive macular hypomelanosis of the trunk: primary acquired hypopigmentation. J Cutan Pathol. 1988;15(5):286-9.
4. Guillet G, Helenon R, Guillet MH, Gauthier Y, Menard N. Progressive and confluent hypomelanosis of the melanodermic metis. Ann Dermatol Venereol. 1992;119(1):19-24.
5. Guillet G, Guillet MH. Creole dyschroma or idiopathic macular hypomelanosis of the melanodermic halfcast of Guillet-Helenon. Bull Soc Pathol Exot. 1997;90(5):333-34.
6. Menke HE, Doornweerd S, Zaal J, Roggeveen C, Dingermans KP, van der Bergh Weerman M, et al. Acquired nummular and confluent hypomelanosis of the trunck. Paper presented at: Second Annual Meeting of the European Society for Pigment Cell Research; June 18-21, 1989; Uppsala, Sweden.
7. Relyveld GN, Dingemans KP, Menke HE, Bos JD, Westerhof W. Ultrastructural findings in progressive macular hypomelanosis indicate decreased melanin production. J Eur Acad Dermatol Venereol. 2008;22(5):568-74.
8. Westerhof W, Relyveld GN, Kingswijk MM, de Man P, Menke HE. Propionibacterium acnes and the pathogenesis of progressive macular hypomelanosis. Arch Dermatol. 2004;140(2):210-4.
9. Relyveld GN, Menke HE, Westerhof W. Progressive macular hypomelanosis: an overview. Am J Clin Dermatol. 2007;8(1):13-9.
10. Wu XG, Xu AE, Song XZ, Zheng JH, Wang P, Shen H. Clinical, pathological, and ultrastructural studies of progressive macular hypomelanosis. Int J Dermatol. 2010;49(10):1127-32.
11. Perman M, Sheth P, Lucky AW. Progressive macular hypomelanosis in a 16-year old. Pediatr Dermatol. 2008;25(1):63-5.
12. Relyveld GN, Kingswijk MM, Reitsma JB, Menke HE, Bos JD, Westerhof W. Benzoyl peroxide/clindamycin/UVA is more effective than fluticasone/ UVA in progressive macular hypomelanosis: a randomized study. J Am Acad Dermatol. 2006;55(5):836-43.
13. Almeida ART, Bedani TP, Debs EAF, Ferreira JAD. Estudo piloto para avaliar a eficácia da minociclina no tratamento da hipomelanose macular progressiva (HMP). Surg Cosmet Dermatol. 2009;1(1):25-28.
14. Wu XG, Xu AE, Luo XY, Song XZ. A case of progressive macular hypomelanosis successfully treated with benzoyl peroxide plus narrow-band UVB. J Dermatolog Treat. 2010;21(6):367-8.
15. Almeida ART, Nei DSY, Almeida JG. Estudo duplo cego randomizado e comparativo entre minociclina e placebo no tratamento da hipomelanose macular progressiva. Surg Cosmet Dermatol. 2011;3(3):219-25.
16. Neynaber S, Kirschner C, Kamann S, Plewig G, Flaig MJ. Progressive macular hypomelanosis: a rarely diagnosed hypopigmentation in Caucasians. Dermatol Res Pract. 2009;2009:607682.
17. Kumarasinghe SP, Tan SH, Thng S, Thamboo TP, Liang S, Lee YS. Progressive macular hypomelanosis in Singapore: a clinico-pathological study. Int J Dermatol. 2006;45(6):737-42.
18. Di Lernia V, Ricci C. Progressive and extensive hypomelanosis and extensive pityriasis alba: same disease, different names? J Eur Acad Dermatol Venereol. 2005;19(3):370-2.
19. Rodríguez-Lojo R, Verea MM, Velasco D, Barja JM. Progressive and confluent macular hypomelanosis. Actas Dermosifiliogr. 2010;101(3):268-9.
20. Lesueur A, Garcia-Granel V, Hélénon R, Cales-Quist D.Progressive macular confluent hypomelanosis in mixed ethnic melanodermic subjects: an epidemiologic study of 511 patients. Dermatol Venereol. 1994;121(12):880-3.
This study was carried out at the Centro de Dermatologia Prof. René Garrido Neves - Fundação Municipal de Saúde de Niterói - Niterói (RJ), Brazil.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}