


Marisa Gonzaga da Cunha1; Ana Lúcia Gonzaga da Cunha2; Marzia Macedo3; Carlos D'Apparecida Machado4
Introduction: Discoloration and grooves are common in the lower eyelid and tend to give the bearer's appearance - even at a young age - an effect of tiredness, advanced age, and deepening of the eyeballs. Aimed at correcting these visual effects, cutaneous filling for local volume restoration has been currently indicated as a treatment, with the proposition of a number of products and techniques. Objective: To describe and evaluate the superficial application technique with the use of a fluid monophasic polydensified hyaluronic acid. Materials and methods: Sixty patients being treated between 2011 and 2014 underwent the technique. The evaluation was carried out by an applicator physician through the comparison of photographs and through questionnaires based on the Hirmand's classification answered by the patients. Results: The applicator physician rated the treatment as excellent (35% of cases), very good (50%) or good (15%), whereas for patients the results were excellent (30%), very good (50%) or good (20%). There were no reports of significant or long-term adverse effects. Conclusion: This superficial subdermal technique is easy to perform, has few adverse effects, and yields good results, leading to a high degree of patient satisfaction.
Keywords: SKIN AGING; HYALURONIC ACID; HYPERPIGMETATION
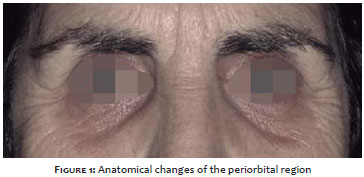
The quest for the prevention or correction of signs of aging in the facial area has motivated the development of new surgical techniques and minimally invasive nonsurgical treatments.1, 2 Special attention has been given to the periocular region, where multifactorial alterations - texture, color and skin firmness, bone resorption, and displacement of soft tissue - lead to the emergence of depigmentation, wrinkles and/or fat pads (Figure 1). According to clinical findings, one therapeutic option alone may not be sufficient.1, 2
One of the main complaints related to the lower eyelid is the tear trough's deformity that, when pronounced, translates into an unsightly depression, lending a tired and aged appearance to one's gaze - even in young patients.3, 4 According to Stutman, one of the most important elements in the aesthetics of the infrapalpebral region is the smooth transition between preseptal and orbital portions of the orbicularis oculi muscle, in continuity with the malar region, without a marked transition line.2
The first reference to infrapalpebral depression dates from 1932, having been described by Whitnall. The expression nasojugal groove was introduced later on by Dukes-elder and Wybar, in 1961. The terms lacrimal canal deformity and tear trough deformity were consolidated by Flowers and Loeb in 1969.2
In its upper portion, the tear trough corresponds to a cutaneous groove that runs obliquely and inferolaterally, from the inner canthus up to about the mid-pupillary line, and can continue laterally along the palpebromalar sulcus (Figure 2). 3, 4, 5 It can be a result of both genetic and anatomical variations present in young individuals and the individual body region's aging process.
The exact anatomical origin of the lacrimal groove remains unclear, with several conflicting reports in the literature.4,5 The references suggest the following as possible causes: (1) the prominence of the orbital border resulting from the downward displacement of the malar fat pad; (2) the orbital septum's anchorage on the orbit's marginal arc, at the inferomedial portion level of the arc; (3) the loss of local fat or the postseptal fat pad herniation; (4) the presence of a triangular cleft limited by the orbicularis muscle of the eye, levator labii superiori alaeque nasi and levator labii superiori muscles; (5) the absence of adipose tissue in the central and medial portions underlying the orbicular muscle in the groove's region.2, 5, 6 Through dissections of cadavers, Haddock et al. correlated the lacrimal groove with the preseptal portion of the orbicularis oculi muscle and the junction of the orbital portions with differences in skin texture and underlying fat. In the deep plane, they found a separation between the tear trough and the palpebromalar junction.4 Wong, Hsieh and Mendelson identified a true osteocutaneous ligament: the tear trough ligament, which they defined as the main etiological factor for the lacrimal groove. This ligament is located between the eyelid and the origins of the orbital portions of the orbicularis oculi muscle. It inserts firmly in the region's skin and originates from the maxillary bone.3
Surgical correction of the lacrimal groove deformity is considered difficult.2 The objective of traditional blepharoplasty is the removal and anchorage of the orbital septum's tissues. However, recent studies of facial aging have highlighted the correction of the local volume losses and not just the removal of tissues. In this way, the idea of infraorbital groove filling for the restoration of the lost volume has arisen.
The first studies reporting the use of fillers in the nasojugal groove date back to 2003 and were carried out by Michel Kane, whose team applied hyaluronic acid more superficially. 6 In 2004, Robert Alan Goldberg described the hyaluronic acid application technique (Restylane®) with a 30G needle under the orbicularis oculi muscle.7 Many application techniques have been described to date. 2, 8, 9
The objective of the present study is to describe the technique for the superficial filling of the lacrimal groove using fluid polydensified monophasic hyaluronic acid, which is indicated for subepidermal or dermal superficial applications, and to describe its safety and effectiveness.
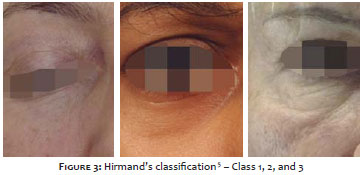
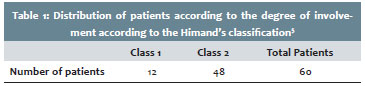
The present paper describes a retrospective study of patients treated by the authors at private practices and at the Cosmetic Dermatology Sector of the Dermatology discipline, at FMABC between 2011 and 2014. Sixty patients aged between 18 and 50 years (mean = 27.6 years), with tear troughs Classes 1 and 2 according to the Hirmand's classification (Figure 3, Table 1) were treated. Fluid polydensified monophasic hyaluronic acid 20 mg/ml Anteis Soft® (Merz Aesthetics, São Paulo, Brazil), indicated to increase the volume of cutaneous tissue with superficial applications, was used. Polydensification provides the product with great integration properties into the dermal tissue, promoting uniform volume increase at the injection site, without the risk of the Tyndall effect.
The employed technique was the superficial subdermal - which allows the visualization of the needle - in retroinjection with a 30G 1/2 (0.3 mm x 13.0 mm) needle, forming "sticks" in the groove line, and subsequent molding of the injected material up until the complete filling of the tear trough. The product amount varied according to the groove's depth (between 0.3 ml and 0.6 ml on each side). Cold compresses were applied before and after the procedure to prevent edema and hematoma. All patients were photographed and analyzed under standardized conditions before the treatment and 30 days after its completion.
The evaluation was performed by the applicator physician using photographic comparisons and the Hirmand's classification questionnaire administered to the patients.
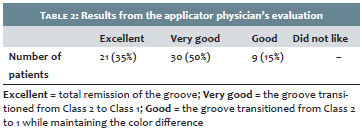
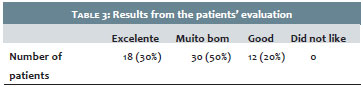
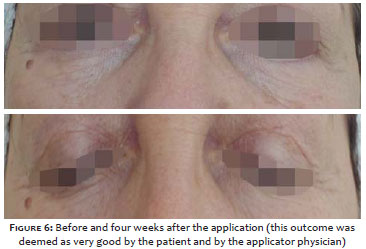
The results presented in this study were observed after a single application and were based on the Hirmand's classification,5 having been rated as excellent by the patients and the applicator physician when there was a total disappearance of the groove; as very good when the groove transitioned from Class 2 to Class 1; and as good when the groove transitioned from Class 2 to Class 1, but maintained the color difference (Figures 4 and 8). There were no cases with an absence of improvement, or with patient or applicator physician dissatisfaction (Tables 2 and 3).
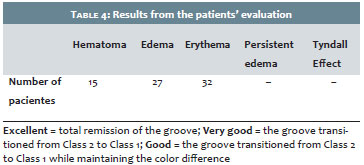
Adverse effects were minor and transient. There were slight hematomas after the application, which could be camouflaged with corrective makeup and which resolved in a few days; transient edema of short duration (about two hours); and immediate local erythema - more frequently observed in patients with skin phototypes I and II. The use of local cooling before and after the application minimizes these complications. There were no cases of persistent edema among the patients treated, and there were no cases of the Tyndall effect (Table 4). The duration of the corrective effect ranged from 9 months (80% of patients) and 12 months (20% of patients).
The skin of the palpebral region is the thinnest on the human body (<1 mm), with the epidermis consisting of a very thin stratified epithelium (0.4 mm) and the dermis also extremely thin, composed of loose connective tissue and virtually absent in the pre-tarsal skin and eyelid's medial and lateral ligaments, where it adheres to the fibrous underlying tissue.
The tear trough consists of a cutaneous groove, which runs obliquely and inferolaterally from the inner canthus to, approximately, the mid-pupillary line, continuing laterally with the palpebromalar sulcus. 2, 3, 4
Diverse techniques are described for its treatment. Several studies mention the use of cutaneous filling, with the discussion focusing on which filler would be more appropriate, since the skin is very thin and vascularized in this region. Among the filling substances, hyaluronic acid stands out as the most suitable due to its application straightforwardness, low allergenic potential and homogeneous texture with good esthetic outcomes, as well as a low risk of complications6, especially using the superficial application technique.
Like any filler, hyaluronic acid has advantages and disadvantages. The advantages are: minimal degree of invasion, straightforward application, low allergenic potential and absence of a need for prior skin test. Furthermore, because of its viscosity, it adapts better to nasojugal contours and provides better esthetic results and a lower risk of complications due to its homogeneous texture.7, 10 Among the disadvantages are: impermanent results, effectiveness for about only nine months and the necessity for topical anesthesia before application.10
The optimal duration observed in patients in the present study may be linked to the replacement of hyaluronic acid, which entails hydric replacement in the dermis with the subsequent increase in thickness, and improvement in turgor, elasticity, and firmness10 as a result of new collagen production.11, 12
Complications include erythema immediately after the application, hematomas, contour irregularities, overcorrection of the groove, persistent malar edema, and color alterations in the periorbital area - all of which occur independently of the filling substance used. The color alterations can be of two types: one that can be observed in patients with prominent dark circles, which after filling procedures in the groove convey the impression of worsening due to the increased exposure of a darkened surface (the patient should be warned about this risk); and another, characterized by the presence of a bluish area due to the superficialization of the filler - known as the Tyndall effect - and which can be observed in people with very fair and thin skin.
Despite being considerably rare, another possible complication described is blindness. In order to avoid the embolization of the ophthalmic artery, some precautions have been described. Among them are: to avoid applying filling substances close to the inner canthus (this region houses the supratrochlear, supraorbital, and dorsal nasal arteries (with the latter being a tributary of the ophthalmic artery); to apply small filler amounts at a time; to inject slowly; to avoid applications in bolus; to apply in more superficial planes or to use blunt tip cannulas.6, 7, 9
The superficial subdermal surface application technique of fluid polydensified monophasic hyaluronic acid suitable for surface applications - as described in the drug description leaflet - lends safety to the application for the correction of the lacrimal groove due to its greater local bio-integration,14 with low risk of contour irregularities and color alterations - such as the Tyndall effect.13 The formation of hematomas can occur in any technique and is a less severe complication in these cases, since it does not entail compression risk to any important structure and may be minimized by applying local cooling before and immediately after the application. With this technique, given that the application is sub-epidermal, there is no risk of arterial obstruction or product migration. The most common complication is overcorrection, though this risk can be minimized with the slow application of the material and the use of a filler with low-density, good moldablility, and good integration into the tissues properties.14
It is worth noting that in cases with significant skin sagging, with the visualization of fat pads, traditional blepharoplasty is indicated for the removal of tissue and correction of the orbital septum. The filling procedure is complementary and indicated only for correcting the loss of local volume.
The superficial subdermal tear trough filling technique is a safe and easy to perform procedure, with a low risk of complications. It is mainly indicated for young patients without cutaneous sagging and as a complementary technique to blepharoplasty in patients who also have tissular laxity, and should be performed after surgical correction.
Hidradenitis is a chronic and recurrent inflammatory disease that affects flexural areas of the skin, such as the armpits, and the inframammary and groin regions.1 It is a painful and often disfiguring condition, which manifests after puberty and is characterized by deep inflammatory lesions in the region of the apocrine glands.2 The prevalence of hidradenitis in the general population is about 1%, affecting more women than men (4:1), and is associated with genetic and hormonal predisposition (androgen excess).2, 3, 4
Hidradenitis initially emerges as an inflammation around the hair follicle, followed by a series of damaging events that lead to a rupture of the follicular infundibulum, forming deep painful nodules and abscesses that generate fistulas and scarring. This sequence of events tends to be recurrent in most patients.3, 5 Thus, hidradenitis may arise in the form of abscesses, folliculitis, pyogenic granuloma, comedones, fistulas, scars, and keloids.6
Given the variety of possible manifestations of this disease, the Hurley's staging system is used to classify the picture into three stages. During Stage I there are one or more separate abscesses, but an absence of fistulae or scars; in Stage II there are one or more separate abscesses, and scarring and fistula formation; and in Stage III there is a confluence of the lesions with interconnected fistulas and abscesses.1, 3 The lesions' pathophysiology involves both follicular innate immunity defect and hyper-reactivity to coagulase-negative staphylococci.6
Hidradenitis can have significant clinical consequences, but most of all it can negatively affect a patient's quality of life.1, 7 The pain picture, the unpleasant odor, and the scars are all factors that have an impact on patients.8 Despite the importance of a treatment to resolve this condition, the current options are limited, and there is a lack of studies involving safe and effective therapies.2
Pharmacological treatments include topical and oral antibiotics, intralesional corticosteroids, hormone therapy, retinoids, immunosuppressants and biological agents. Surgical treatments vary from drainage and incision procedures to debridement and a wide surgical excision of fistulas and abscesses. Most recently, there have been reports of the use of technologies such as diode laser, CO2 laser, Nd:YAG (Neodimiun:Yttrium Aluminum Garnet) and photodynamic therapy with good results in the treatment of hidradenitis.1, 3, 8, 9
Due to the success of some laser types in hidradenitis, the authors sought to evaluate the use of a new technology, the 1,340nm Nd:YAP (Neodimiun:Yttrium Aluminum Perovskite). This laser was effective in the treatment of inflammatory acne through the organization of the collagen fibers and reduced inflammatory infiltrate.10 Thus, since it is also a chronic inflammatory disease, the authors sought to obtain positive results in the treatment of hidradenitis with 1,340nm ND:YAP.
Three female patients, all bearers of hidradenitis at Hurley's Stages I or II, who were being treated at the Dermatology Ambulatory of the Faculdade de Medicina de São Jose do Rio Preto (FAMERP), were selected. The patients had already undergone drug treatments without success. They did not use systemic or topical therapy for three weeks and had not undergone previous surgical treatment. The diagnosis of pregnancy was excluded for the three patients. The study was approved by the Research Ethics Committee of FAMERP.
In a prospective study, the patients underwent four 1,340nm ND:YAP laser sessions (Etherea®, Industra Technologies Indústria e Comércio Ltda., São Carlos, São Paulo, Brazil), with the following parameters: 100mJ, 100mtz and 8mm tip. The interval between sessions was one month. The response to the treatment was assessed through a comparison of photographs taken prior to and one month after the fourth laser therapy session.
Two dermatologists unrelated to the study compared the photographs and classified them as follows: 0 - worsening, 1 - lack of improvement, 2 - moderate improvement, and 3 - significant improvement. Each patient's degree of satisfaction was evaluated based on a rating scale of: 0 - unsatisfied; 1 - somewhat satisfied; 2 - satisfied; and 3 - very satisfied.
The objective analysis of the photographs carried out by dermatologists unrelated to the study was rated with "significant improvement" of the inflammation in all cases (Figures 1 and 2). The three patients were very satisfied with the outcome and showed only mild erythema and pain as adverse effects to the treatment. During the six months following the treatment, none of the patients had a recurrence.
A chronic inflammatory process with significant lymphocytic inflammatory infiltrate and disorganization of collagen fibers was observed in a histological examination performed prior to the treatment (Figures 3 and 4). After the treatment, however, a significant reduction of the inflammatory infiltrate and organization of collagen fibers became apparent (Figures 5 and 6).
Hidradenitis is a chronic inflammatory disease that adversely affects a patient's quality of life and is associated with clinical morbidity. Nevertheless, there is a lack of effective and permanent treatment for this disease, since recurrences are frequent1,11 Laser treatment has the advantage of being restricted to the affected body site and not being associated with systemic side effects.3
1,064nm ND:YAG laser (Neodymium:Yttrium Aluminum Garnet) laser has recently shown good results in the treatment of hidradenitis.1, 3, 12, 13 According to Mahmoud et al. 2010,3 it is likely that the mechanism of action responsible for the therapeutic success is the follicular ablation and destruction of inflammatory lesions through selective photodermolysis.
In the present study, the authors describe the unprecedented success of 1,340nm Nd:YAP laser to treat hidradenitis. This technology has already proven effective in the treatment of inflammatory acne, with possible similar action in fibrosis and inflammation, which also characterize the hidradenitis. 10 Thus, it was possible to guarantee satisfaction to patients and approval from a medical point of view, confirming this therapy's efficacy in the histological examination.
The action of 1,340nm Nd:YAP in hidradenitis lesions (Stages I and II) was demonstrated to be durable, with no recurrence reported within the six months following the treatment. Side effects were minimal and localized. Therefore, the authors sought a safe and effective therapeutic alternative in the face of a condition having a great impact on the patient.
Since it is a case of a pathology associated with functional, aesthetic, and psychological damage, hidradenitis calls for effective therapeutic methods. In the present study, the authors conclude that 1,340nm Nd:YAP laser was effective and safe in three patients with hidradenitis, presenting a new therapeutic modality for the condition. Further studies on the different hidradenitis stages and with longer follow up are necessary. 1
1. Moran ML. Office-based periorbital rejuvenation. Facial PlastSurg. 2013;29(1):58-63.
2. Stutman RL, Codner MA. Tear trough deformity: review of anatomy and treatment options. Aesthet Surg J. 2012;32(4):426-40.
3. Wong CH, Hsieh MKH, Mendelson B. The tear trough ligament: anatomical basis for the tear trogh deformity. Plast Reconstr Surg. 2012;129(6):1392-402.
4. Haddock NT, Saadeh PB, Boutros S, Thorne CH. The tear trough and lid/cheek junction: anatomy and implications for surgical correction. Plast Reconstr Surg. 2009;123(4):1332-1340.
5. Hirmand H. Anatomy and nonsurgical correction of the tear trough deformity. Plast Reconstr Surg. 2010;125(2):699-708.
6. Kane MAC. Treatment of tear troug deformity and lower lid bowing with injectable hyaluronic acid. Aesth Plast Surg. 2005;29(5):363-67.
7. Goldberg RA, Fiaschetti D. Filling the periorbital hollows with hyaluronic acid gel: initial experience with 244 injections. Ophthal Plast Reconstr Surg. 2006;22(5):335-41; discussion 341-3.
8. Braz AV, Aquino AO. Preenchimento do sulco nasojugal e da depressão infraorbital lateral com microcânula 30G. Surg Cosmet Dermatol. 2012;4(2):178-81.
9. Steinsapir KD, Steinsapir SMG. Deep-fill hyaluronic acid for the temporary treatment of the naso-jugal groove: a report of 303 consecutive treatments. Ophthal Plast Reconstr Surg. 2005;22(5):344-8.
10. Bosniak S, Sadick NS, Cantisano-Zikha M, Glavas IP, Roy D. The hyaluronic acid push technique for the nasojugal groove. Dermatol Surg. 2008;34(1):127-31.
11. Wang F, Garza LA, Kang S, Varani J, Orringer JS, Fisher GJ, Voorhees JJ. In vivo stimulation of de novo collagen production caused by cross-linked Hyaluronic Acid dermal filler injections in photodamaged human skin. Arch Dermatol. 2007;143(2):155-163.
12. Fisher GJ, Varani J, Voorhess JJ. Looking older: fibroblast collapse and therapeutic implications. Arch Dermatol. 2008;144(5):666-72.
13. Micheels P, Sarazin D, Besse S, Sundaran H, Flynn T. A Blanching Technique for Intradermal Injection of the Hyaluronic Acid Belotero. Plast Reconstr Surg. 2013;132(4 Suppl 2):59S-67S.
14. Tran C, Carraux P, Micheels P, Kaya G, Salomon D. In vivo Bio-Integration of Three Hyaluronic Acid Fillers in Human Skin: A Histological Study. Dermatology. 2014;228(1):47-54.
This study was carried out at a private practice and at the Cosmetic Dermatology Sector of the Dermatology discipline, Faculdade de Medicina do ABC (FMABC) - Santo André (SP), Brazil.
 All content the journal, except where identified, is under a Creative Commons Attribution-NonCommercial 4.0 International license - ISSN-e 1984-8773
All content the journal, except where identified, is under a Creative Commons Attribution-NonCommercial 4.0 International license - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}