


Leandra d'Orsi Metsavaht1; Carlos Alberto Rios Garcia2
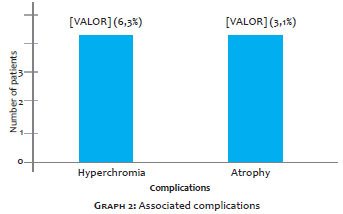
Introduction: The treatment of keloids and hypertrophic scars are an everyday challenge for the dermatologist. Despite the existence of a large therapeutic armamentarium, a variable rate of effectiveness, side effects, and recurrences make it difficult to achieve satisfactory results. As an isolated or in-combination therapy, 5-fluorouracil has the potential to be a part of the treatment paradigm for hypertrophic and keloid scars. Objective: To evaluate, during 12 years, the outcomes of the use of 5-FU (50 mg/ml) in a ratio of 9:1 with triamcinolone acetonide (20 mg/ml) in patients bearing keloids and hypertrophic scars. Methods: Retrospective study of 32 patients with keloids, hypertrophic scars, and cicatricial fibrosis who underwent 1 to 17 intralesional injections of a combination of 5-FU and triamcinolone acetonide in fortnightly intervals. A visual analog scale (VAS) was employed to evaluate the pain/discomfort caused by the lesion, as well as to assess the patient's perception of the scar when seeing it in the mirror. Results: In the comparison of the visual analogue scales (VAS) after the treatment, there was a significant reduction in the level of pain/discomfort (VAS pain) (p = 0.001) and in the assessment of the scar's appearance in the mirror (VAS mirror) (p <0.001). Three patients (9.4%) had complications: hyperchromia (two patients = 6.3%) and atrophy (one patient = 3.1%). Conclusions: 5-FU injections in hypertrophic scars, keloids, and fibroses was found to be a minimally invasive, cost effective, and easily reproducible therapeutic approach with consistent results, which does not invalidate or preclude other techniques.
Keywords: CICATRIX, HYPERTROPHIC; FLUOROURACIL; KELOID
Scars are the result of a natural physiological process of skin repair after injury. When an imbalance occurs at some stage of this process, keloids or hypertrophic scarring may occur which, in addition to being unsightly, often cause pruritus, pain, and contractures. Therefore, excessive scarring can dramatically affect an individual's quality of life, both physically and psychologically, stimulating the search for a treatment. 1, 2
There are marked clinical and histological differences between keloids and hypertrophic scars. A keloid is characterized by an excessive growth of the dense fibrous tissue extending beyond the original borders of the wound, which does not regress spontaneously, tends to recur after excision, and affects up to 16% of the population having African ancestry. 1 Some authors define keloids as "confused scars that do not know how to stop growing." 3 On the other hand, hypertrophic scars can occur in up to 70% of surgical scars and are equally uncomfortable, but remain confined to the borders of the lesion and tend to regress spontaneously in a few years. 1
The proliferation and migration of fibroblasts have a major role in cutaneous healing. The main function of fibroblasts is the synthesis of collagen, proteoglycans, and elastin. Keloids and hypertrophic scars remain in the proliferative phase for a longer period, leading to exacerbated extracellular matrix deposition. 4
Evidence suggests that a propensity for the formation of keloids is autosomal dominant, autosomal recessive, or X-linked with a recessive pattern of inheritance. Nevertheless, the exact incidence and its genesis remain uncertain. 5
Hypertrophic scars and keloids can result from almost any cutaneous trauma, such as acne, burns, minor cuts from shaving, ear or body piercings, or surgical scars. Treatment of keloids can be quite frustrating to both the dermatologist and the patient, for they have a high recurrence rate, as a result of the fact that the new wound will be prone to the same genetic, immunological, biochemical and mechanical mechanisms as the initial wound. 6-8
Literature reports indicate a recurrence rate ranging from 45-100% when the simple excision of keloids is performed. When associated with intralesional injections of corticosteroids, total recurrence falls to a level between 37-50%. The association of radiotherapy minimizes this level to 10% in the first 48 hours of the post-operative period.6-10 One study showed that electron beam irradiation is superior to betatherapy for the treatment of operated keloids, due to better distribution in the tissue. 11
Cryosurgery uses repeated cooling and heating of the tissue, inflicting vascular damage that leads to anoxia and, ultimately, to cell death. The success rate reported in studies in which as much contact as liquid nitrogen spray were used ranged from 32- 74% after two or more sessions, with better responses in hypertrophic scars when compared to keloids. Its use, however, is limited to small scars. The main adverse effects are hypo- or hyperpigmentation, blistering, and post-operative pain.12-14 More recently, an intralesional needle adapted to the cryosurgery device showed increased efficacy when compared to the contact/ spray treatment, providing a shorter reepithelialization period. 15
Several studies have investigated antineoplastic agents and there seems to be a marked improvement in recurrence rates, patient satisfaction, and overall quality of scars when these agents are used. Intralesional injection and/or irrigation with interferon α2b, interferon-γ, mitomycin-C, bleomycin or 5-FU seems to have a positive effect in the reduction of pathological scars. There is plenty of evidence that these drugs used in isolation or in combination therapies have the potential to be an integral part of the paradigm for the treatment of hypertrophic scars and keloids. 16
Mitomycin has been highly effective for topical use after the shaving of keloids. 17
Some authors suggest that novel therapies do not hit the target when it comes to the treatment of pathological scarring, leading to worse than expected results. They propose that mTOR (mammalian target of rapamycin) be used as the new target for blocking fibroproliferation. In a study containing the analysis of the fibroblasts' genome, hypertrophic scars and keloids showed an exacerbated expression of collagen type I and II, which was effectively neutralized by the use of rapamycin. 18
Bleomycin sulfate is an antineoplastic agent that directly inhibits collagen synthesis by decreasing the stimulus via TGFß1. It was first studied in 1990 as a scar reducing agent. After three to five intralesional bleomycin injection sessions during one month, the authors observed a keloid reduction rate of 69.4%. Subsequent studies revealed similar results, with a significant improvement in the height and flexibility of keloids and hypertrophic scars, as well as a reduction of erythema, pruritus, and pain. Occasionally there was hyperpigmentation and dermal atrophy. Due to its toxicity, it is necessary to be on the lookout for side effects, although they are typically uncommon. Clinical studies on its effectiveness and additional investigations are needed before it can be included in treatment protocols. 19
Corticosteroids inhibit the healing process in three ways: i) by suppressing local inflammation through the inhibition of the migration of leukocytes and monocytes, and phagocytosis; ii) because they are potent vasoconstrictors that reduce local oxygenation; iii) because their antimitotic effect inhibits keratinocytes and fibroblasts, thereby reducing re-epithelialization and new collagen formation. For these reasons, the intralesional injection of corticosteroids is often related to the atrophy of the scar and surrounding tissues, telangiectasia formation, and a high rate of recurrence. 19
One antineoplastic drug of the pyrimidine analogs class is 5-fluorouracil (5-FU), which is capable of inhibiting the biosynthesis of pyrimidine nucleotides or mimic natural metabolites, thereby interfering with the synthesis of nucleic acids. It effectively inhibits both the thymidylate synthesis (which is an essential precursor of DNA synthesis for cell division) and the processing of RNA and protein synthesis. 20 These characteristics lend it an important role in the treatment of malignant tumors of epithelial origin, such as the colorectal tumor, 8 and in the topical treatment of premalignant skin lesions, such as actinic keratosis. 7 For characteristically inhibiting the proliferation of fibroblasts, having a wide therapeutic window, and being easy to handle, it has been used since 1990 in surgeries for glaucoma filtering (in which exacerbated healing can compromise the surgical outcome) 21-22 and in the repair of the flexor tendons of the hand (since excessive scarring often causes adhesions and limits functional results). 23-25
In 1999, Richard Fitzpatrick published a review article in the journal Dermatologic Surgery with a description of his nine years of experience using 5-FU in more than a thousand patients with sequelae of hypertrophic scars and keloids resulting from surgery, acne, and burns. His observation was subjective, however the incidence of positive results and patient satisfaction were noteworthy and have yielded 258 citations of his article to date. Fitzpatrick noted that not all injection sessions resulted in an obvious clinical improvement, however it was rare that scars did not respond favorably. In general, the more inflamed, more symptomatic, more firmly hardened and red scars responded better. Scars that were several years old and still very firmly hardened, although not inflamed or symptomatic, responded significantly less well. With repetitive injections, scars became softer and more flattened. 26
A retrospective study was carried out to evaluate 5-FU's clinical results and complications when used for treating keloids, hypertrophic scars, and scarring fibrosis, by surveying records corresponding to a period of 12 years. The parameters used were: 1) photographic comparison, 2) visual analog scale (VAS) to assess the intensity of pain and/or spontaneous discomfort, 3) patients' self-assessment of the aesthetic impression of their lesions, also through VAS.
A survey of the records of 44 patients was carried out at the Plastic and Reconstructive Hand Surgery of the 11ª Enfermaria da Santa Casa da Misericórdia do Rio de Janeiro (2003-2004) and at one of the author's private practice (LDM 2003-2014). The patients had undergone treatment for keloids, hypertrophic scars, and scarring fibrosis, with intralesional injections of 5-FU. Of the 44 patients treated, one was excluded due to complaint of severe pain during the procedure, and a further 11 due to non-participation after the 1st session. The development of the lesions ranged from one month to 10 years.
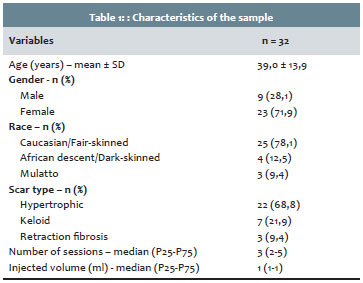
The sample consisted of 32 patients aged from 11 to 73 years (mean age = 39 ± 13.9 years). There was a predominance of female (71.9%) and Caucasian (78.1%) patients, and hypertrophic scars (68.8%), as shown in Table 1.
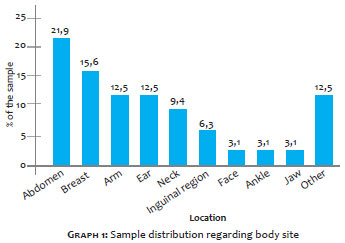
The four most common body sites were the abdomen (21.9%), breast (15.6%), arm (12.5%) and ear (12.5%), as can be seen in Graph 1.
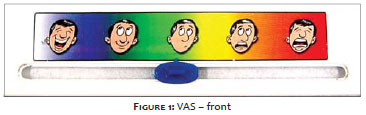
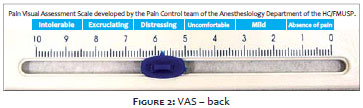
The lesions were photographed before, during, and after the treatment. The analog visual scale (VAS) was used due to the fact that the authors deemed it easy to understand and use. It was employed to assess the intensity of pain and/or spontaneous discomfort, and in the self-evaluation of the aesthetic impression of a patient's own lesion when visualized in the mirror (VAS pain/discomfort and VAS "at the mirror") (Figures 1 and 2).
Another widely used scale that is related to the lesions' clinical characteristics is the Vancouver scale (Vancouver Scar Scale - VSS), also known as the Burn Scar Index, which requires precision equipment for the determination of some measures. 27
The drug was prepared with a mixture of triamcinolone acetonide and 5-FU in the ratio of 1:9 (0.1-ml of 20-mg/ml triamcinolone for each 0.9 ml of 50-mg/ml 5-FU). The injections were performed with 13 mm long needles and 30G internal diameter, and syringes with a 1 ml or 3 ml body, depending on the volume needed for the lesion's size, in fortnightly intervals up until a clinical and aesthetic satisfaction were achieved or there was an interruption due to mutual decision between patient and physician in a case where the treatment was not considered effective. The median values for the number of sessions and injected volumes was 3 (percentiles 25-75:2-5) and 1 ml (percentiles 25-75:1-1), respectively. The follow-up period ranged from 1 to 8.5 months.
The solution was injected into the tissular mass of hypertrophic scars and keloids and in areas of fibrosis (hardened tissue) up until whitening was achieved with an average volume of 0.05 ml per injection point in the hardened area of the scar. Depending on the lesion's size, multiple injection points may be necessary. In such cases it is important to attempt to distribute the points with a distance of about 1 cm between them.
Statistical analysis
Quantitative variables were expressed as mean values and standard deviations or medians and interquartile range. The normality was assessed using the Shapiro-Wilk test.
The Wilcoxon test was used to compare pre- and post-treatment results. The correlation between the continuous variables was assessed using the Spearman's rank correlation coefficient. In the comparison between groups, the Mann-Whitney U test and Kruskal-Wallis tests were applied.
The significance level was 5% (p < 0.05), and analyses were performed using the SPSS version 21.0 software.
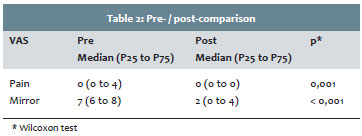
In the visual analogue scales (VAS) comparison after treatment, there was a significant reduction in spontaneous pain levels associated with lesions (VAS pain) (p = 0.001) as well as in the scar's aesthetic analysis when evaluated in the mirror (VAS mirror) (p <0.001), as presented in Table 2.
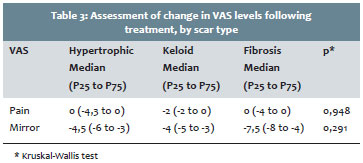
The changes in the VAS scales after the treatment, according to the type of scar are shown in Table 3 showed no significant difference between the diverse types of scarring (p>0.20).
There was no statistically significant correlation between age, gender, scar type, location, and number of sessions and injected volume, with the decrease in the levels of both pain and mirror-based evaluation (p> 0.10).
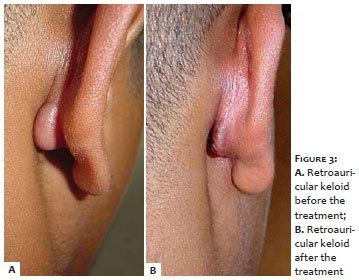
The seven patients with keloids had both clinical and aesthetic improvements. (Figure 3) Of these, one returned after six years presenting recurrence. The two patients who had serious sequelae from burns and presented fibrotic scar retraction in the neck, hands, and armpit areas that caused a restriction of motion amplitude, had an important improvement in the range of motion and functionality for everyday activities, and a decrease in discomfort/pain (Figure 4).
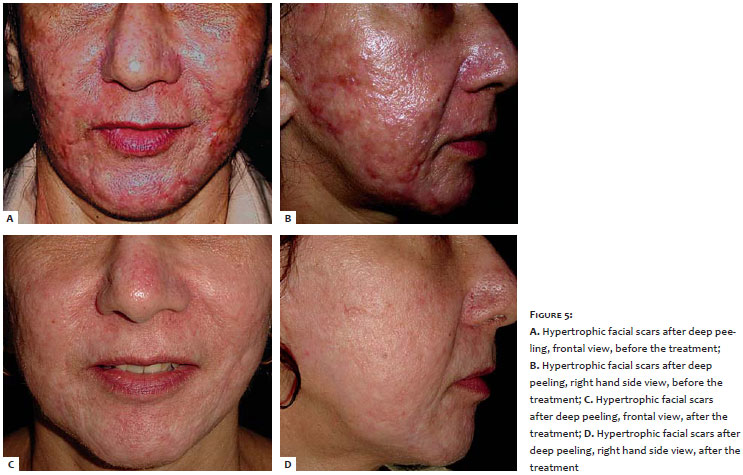
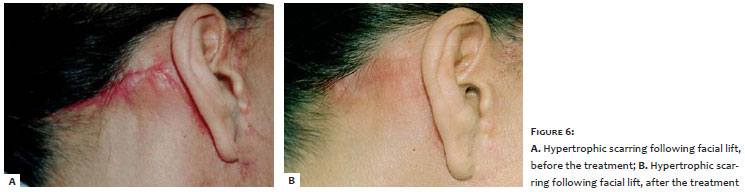
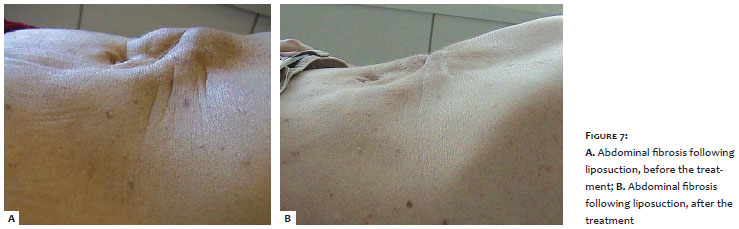
Of the 22 Caucasian patients with varied hypertrophic scars (Figures 5 and 6), only one did not show satisfactory clinical or aesthetic improvement. The three who had cicatricial fibrosis had improvement (Figure 7).
Complications or adverse events
All patients improved spontaneously in six months to one year.
Three patients had complications (9.4%): two had hyperchromia (6.3%), and one atrophy (3.1%) (Graph 2).
Pain, burning, or burning sensation was constant in 100% of cases during application, but with different intensities. However there were no reports of persistence of these symptoms in the hours or days that followed the infiltration. Regional erythema was frequent, but also receded spontaneously after a few hours.
Despite the variety of treatment options, such as retinoids, irradiation, intralesional corticosteroids, cryosurgery, silicone gel, pressure, surgery and new modalities like pulsed dye laser, interferon α2β and other antineoplastic agents, there is great difficulty in treating cicatricial lesions. The effectiveness, as well as side effects of these treatments, is variable. 28
Most literature reports on the use of 5-FU injections involve cases that were carried out in keloids.28-33 There were no descriptions of its use in patients with cicatricial fibrosis, therefore the three cases described in the present study were the first to be published. In the two patients with keloid and retraction due to burn sequel, the greatest benefit was the increase in the amplitude of motion and improved joint function. Normally, these results would only be obtained with extensive surgery and rotation flaps or skin grafts.
The cases with the greatest satisfaction index were those involving hypertrophic scars with few local symptoms, since there was an improvement of the erythema and a flattening of the scar, which compares to Fitzpatrick's findings.26 Nevertheless, these outcomes were not statistically significant in the present study. This may have been due to the fact that most patients present with hypertrophic scars.
Patients with fibrosis also noticed that the tissue became looser and that the fibrosis' retraction decreased considerably. In these cases, one very rewarding outcome was that of a patient whose nipple had retracted after surgical placement of breast implants. Another was that of a significant retraction of a scar following an appendectomy. However the most interesting case was that of a patient who developed a considerably hard fibrosis in the mesogastrium (7 cm x 6 cm), after an abdominal liposuction. As the series of sessions progressed, all lesions invariably softened and were easier to inject, while at the same time the pain of the procedure minimized. All three cases had 100% improvement.
The first signs of response were decreased pain and pruritus, followed by the softening of the scar, flattening, and decreased erythema. For Fitzpatrick, a few scars seemed not to respond when injected once every two to four weeks, nevertheless they dramatically responded to the twice or three times a week treatment.26 The authors made a decision to proceed with a fortnightly frequency in their patients.
The authors noticed that the hypertrophic scars responded better than the keloids and that the sooner the treatment began the better the scar's involution, confirming some authors' findings. There was no emergence of telangiectasia.
Excessive pain may have been the reason that some patients dropped out of the treatment after only one application, however it should be taken into consideration that several cases that were followed up with had a satisfactory improvement after just one application. Several authors have reported pain during infiltration in virtually all patients,26, 28, 29, 33 except for Apikian, and Goodman,30 and Sadeghina,31 who performed local anesthetic blocks before the injection. Fitzpatrick 26 attempted to add 2% lidocaine to 5-FU, hoping to thereby lessen the discomfort, however, as the most significant pain is linked to the acute expansion of a hardened tissue, he deemed it inefficient. He then began testing blends containing 10-mg/ml triamcinolone acetonide, up to a ratio of 1:9, which he considered ideal, with less pain and greater effectiveness. The authors of the present study observed something similar, nevertheless they concluded that the less uncomfortable manner to carry out the infiltration is by skillfully performing a puncture in the chosen point and pushing the syringe's plunger very slowly so that the tissues distends slowly. Therefore, the smaller the barrel of the syringe, the greater the control that the applicator has over the pressure of the fluid being injected in the skin. Another variable consistent with the drop out rate is that some patients are originally from very disadvantaged communities and may have had difficulty following the treatment plan due to the travel distance or work restrictions.
Apikian and Goodman30 used 3 mg betamethasone acetate in suspension and 3.9 mg betamethasone sodium phosphate solution at a ratio of 1:4 to 5-FU in both cases. Other authors have used triamcinolone acetate (TA). Gupta, 29 Nanda and Reddy,28 and Sadeghina31 used 5-FU without corticosteroids. In 2007, a double-blind study compared patients using only TA and another twenty using TA + 5-FU, demonstrating that the combination was more effective in the treatment of keloids and hypertrophic scars, in a 12-week follow up. 33
The maximum daily dose of 5-FU recommended for rapid infusion in chemotherapy varies from 800 mg 20 to 1.500 mg, 26 according to the opinions of different authors. Assuming that each syringe with a 1 ml barrel and with a proportional dilution of 1:9 contains 45 mg of 5-FU, 18 to 33 syringe-doses would be necessary to achieve the maximal dose. With the exception of extensive lesions due to burns, a dose of 20 mg to 45 mg per session is in general sufficient for the treatment of scars, therefore with a very wide and safe therapeutic window. This fact is also reflected in a significant way by the cost of the treatment. Currently, a 10 ml vial costs about R$ 18.00 (roughly US $6.05, at the time this paper was published), therefore each syringe-dose containing 0.9 ml 5-FU costs R$ 1.62 (roughly US $0.54, idem). The most limiting factor to its use is perhaps having access to the drug. It is usually only available through large distributors of hospital drugs, which make their supply available only for official institutions or wholesale purchase. Alternatively, the drug can be requested at oncology centers.
In 2011, Sadeghina31 used a technique called 5-FU "tattooing", employing micropunctures, and reported no adverse effects.
The present study's results are very positive if compared to those previously reported with 5-FU and other isolated ones, such as intralesional corticosteroid injections (50-100%), cryo-surgery (60-75%), radiation (72-92%), 585nm pulsed dye laser (57-83%).28
There were no cases of ulceration in up to 21% of cases, as already reported by the authors. 28
As suggested by Fitzpatrick 26 and Alster, and Handrick, 34 intralesional injections of 5-FU also have the advantage that they can be combined with other treatments, such as intralesional corticosteroids, laser, and cryosurgery, for the optimization of results. This may also reduce the duration of the treatment as well as the side effects related to a prolonged treatment employing just a single therapy.
Intralesional injection of 5-FU remain as a safe and effective alternative for the treatment of hypertrophic, fibrous, painful, and unsightly scars or those causing a functional limitation. This is a minimally invasive, cost effective, and easy to reproduce therapeutic approach that has consistent results and does not invalidate or preclude other approaches in case of failure.
The authors of the present study would like to thank Dr. Joseph Gervais (Head of Plastic and Reconstructive Hand Surgery of the 11ª Enfermaria da Santa Casa da Misericórdia do Rio de Janeiro), and Dr. Bogdana Victoria Kadunc (S&CD's Chief/Head Editor) for all the encouragement and support for the publication of this study.
1. Gauglitz GG, Korting HC, Pavicic T, Ruzicka T, Jeschke MG. Hypertrophic Scarring and Keloids: Pathomechanisms and Current and Emerging Treatment Strategies. Mol Med. 2011;17(1-2):113-25.
2. Furtado F, Hochman B, Ferrara SF, Dini GM, Camelo-Nunes JM, Juliano Y, et al. What factors affect the quality of life of patients with keloids? Rev Assoc Med Bras. 2009;55(6): 700-4.
3. Narakula GK, Shenoy RK. A prospective clinical review of "multi model" approach for treating ear keloids. Indian J Plast Surg. 2008;41(1): 2-7.
4. Al-Attar A, Mess S, Thomassen JM, Kauffman CL, Davison SP: Keloid pathogenesis and treatment. Plast Reconstr Surg. 2006;117(1):286-300.
5. Clark JA, Turner ML, Howard L, Stanescu H, Kleta R, Kopp JB. Description of familial keloids in five pedigrees: evidence for autosomal dominant inheritance and phenotypic heterogeneity. BMC Dermatol. 2009;9:8
6. Mustoe TA, Cooter RD, Gold MH, Hobbs FD, Ramelet AA, Shakespeare PG, et al. International Clinical Recommendations on Scar Management. Plast Reconstr Surg. 2002;110(2):560.
7. Kadunc B, Palermo E, Addor F, Metsavaht L, Rabello L, Mattos R, et al. Tratado de cirurgia dermatológica, cosmiatria e laser da Sociedade Brasileira de Dermatologia. Rio de Janeiro: Ed. Elsevier; 2012.
8. Robinson JK, Hanke WC, Siegel DM, Fratila A. Surgery of the Skin. Philadelphia: Elsevier; 2010.
9. Contin LA, Bastazini Jr I, Alves CJM, Nassif PW, Nascimento DC. Queloides em orelhas: seguimento de 41 pacientes submetidos à cirurgia e infiltração com corticosteróides Keloids in the ears: follow-up of 41 patients who had surgery and intralesional corticosteroid injections. Surg Cosmet Dermatol. 2011;3(2):109-11.
10. Oliveira Junior B, Schellini SA, Lastória JC, Carvalho LR, Stolf HO, Oliveira ALP .Tratamento de quelóides usando radioterapia pós-operatória com elétrons: estudo comparativo e randomizado com dois esquemas. Surg Cosmet Dermatol. 2013;5(1):1626.
11. Batista de Oliveira Jr B, Lastória JC, Pereira HR, Silveira LVAS, Oliveira LP,Stolf HO. Estudo comparativo entre o tratamento radioterápico com elétrons e betaterapia, após cirurgia de queloides. Surg Cosmet Dermatol. 2009;1(2):53-57.
12. Ciampo E, Iurassich S. Liquid nitrogen cryosurgery in the treatment of acne lesions. Ann Ital Dermatol Clin Sper. 1997;51:67.
13. Zouboulis C, Blume U, Buttner P, Orfanos CE. Outcomes of cryosurgery in keloids and hypertrophic scars: A prospective, consecutive trial of case series. Arch Dermatol. 1993;129(9):1146.
14. Ernst K, Hundeiker M. Results of cryosurgery in 394 patients with hypertrophic scars and keloids. Hautarzt. 1995;46(7): 462.
15. Luz FB, Bus LB. Tratamento de queloides por criocirurgia intralesional: proposição de acessório de baixo custo. Surg Cosmet Dermatol. 2011;3(2):109-11.
16. Shridharani SM, Magarakis M, Manson PN, Singh NK, Basdag B, Rosson GD. The emerging role of antineoplastic agents in the treatment of keloids and hypertrophic scars: a review. Ann Plast Surg. 2010;64(3):355-61.
17. Seo SH, Sung HW. Treatment of keloids and hypertrophic scars using topical and intralesional mitomycin C. J Eur Acad Dermatol Venereol. 2012;26(5):634-8.
18. Wong VW, You F, Januszyk M, Gurtner GC, Kuang AA. Transcriptional profiling of rapamycin-treated fibroblasts from hypertrophic and keloid scars. Ann Plast Surg. 2014;72(6):711-9.
19. Gauglitz GG, Korting HC, Pavicic T, Ruzicka T, Jeschke MG. Hypertrophic Scarring and Keloids: Pathomechanisms and Current and Emerging Treatment Strategies. Mol Med. 2011;17(1-2):113-25.
20. Hardman JG, Gilman AG, Limbrid LE. Goodmann &Gilman's The Pharmacological Basis of Terapeutics. 9th ed. New York: McGraw- Hill; 1996.
21. Five year follow-up of the fluorouracil filtering surgery study. The Fluorouracil Filtering Surgery Study Group. Am J Ophthalmol. 1996;121:349-66.
22. Skuta GL, Parrish RK II. Wound healing in glaucoma filtering surgery. Surv Ophthalmol. 1987;32:149-70.
23. Lee DA, Shapourifar-Tehrani S, Kitada S. The effect of 5-fluorouracil and cytarabine on human fibroblasts from Tenon's capsule. Invest Ophthalmol Vis Sci. 1990;31(9):1848-55.
24. Jemec B, C. Linge C, Grobbelaar AO, Smith PJ, Sanders R, McGrouther DA. The effect of 5-fluorouracil on Dupuytren fibroblast proliferation and differentiation. Chir Main. 2000;19(1):15-22.
25. Ketchum LD, Donahue TK. The injection of nodules of Dupuytren's disease with triamcinolone acetonide. J Hand Surg Am. 2000;25(6):1157-62.
26. Fitzpatrick RE. Treatment of inflamed hypertrophic scars using intralesional 5-FU. Dermatol Surg. 1999;25(3):224-32.
27. Baryza MJ, Baryza GA. The Vancouver Scar Scale: an administration tool and its interrater reliability. J Burn Care Rehabil. 1995;16(5):535-8.
28. Nanda S, Reddy BS. Intralesional 5-FU as a treatment modality of keloids Dermatol Surg. 2004;30:54-7.
29. Gupta S, Kalra A. Efficacy and safety of intralesional 5- fluorouracil in the treatment of keloids. Dermatology. 2002;204:130-2.
30. Apikan M, Goodman G. Intralesional 5-fluorouracil in the treatment of keloid scars. Australas J Dermatol. 2004;45(2):140-3.
31. Sadeghinia A, Sadeghinia S. Comparison of the Efficacy of Intralesional Triamcinolone Acetonide and 5-Fluorouracil Tattooing for the Treatment of Keloids. Dermatol Surg. 2012;38:104-9.
32. Guimarães COZ, Parada MB, Bagatin E. Tratamento de quelóide: comparação entre infiltrações intralesionais com 5-fluorouracil, corticosteroide e 5-fluorouracil associado a corticosteróide/Keloid treatment: comparative intralesional injections of 5-fluorouracil, corticosteroid and 5-fluorouracil combined with corticosteroid. Surg Cosmet Dermatol. 2011;3(1):60-2.
33. Darougheh A, Asilian A, Shariati F. Intralesional triamcinolone alone or in combination with 5-fluorouracil for the treatment of keloid and hypertrophic scars. Clin Exp Dermatol. 2007;34(2):219-23.
34. Alster TS, Handrick C. Laser treatment of hypertrophic scars, keloids, and striae. Semin Cutan Med Surg. 2000;19(4):287-92.
This study was carried out at the Plastic and Reconstructive Hand Surgery of the 11ª Enfermaria da Santa Casa da Misericordia do Rio de Janeiro (2003-2004) and at a private practice (LDM 2003-2014) - Rio de Janeiro (RJ), Brazil.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}