


Letícia Arsie Contin1; Daniela Menezes Costa2; Diego Leonardo Bet1; Lucas Bezerra Moura3; Alexandre Ozores Michalany4; Nilton Di Chiacchio5
Keywords: DERMABRASION; LICHENOID ERUPTIONS; ALOPECIA.
Lichen planus pigmentosus (LPPig) is an uncommon
variant of lichen planus (LP). It is clinically represented by brownish, reticular, asymptomatic, or pruritic stains, usually found in areas exposed to sunlight and flexures.1
It represents a therapeutic challenge due to poor response to topical and systemic treatments.2
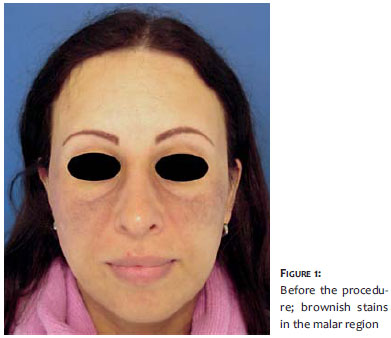
A 38-year-old Caucasian, light-skinned female bearing erythematous macules for 4 years sought dermatological care. The macules had become brownish in the zygomatic region, and were associated with the low density of hairs of the eyebrows (Figure 1). The patient was initially treated with a triple whitening formula (4.00% hydroquinone, 0.05% tretinoin, 0.01% fluocinolone acetonide) and photoprotection. Despite the treatment there was an increase in the intensity and staining of the lesions and a biopsy was indicated with diagnostic hypotheses of melasma, ochronosis and lichen planus pigmentosus (LPPig). Pathology showed interface dermatitis with pigmentary incontinence (Figure 2), compatible with LPPig.3 Due to the poor response to the clinical treatment, and the impact on the patient's quality of life, the authors chose to carry out dermabrasion in a small test area, obtaining good results. They subsequently performed the treatment of all the affected area using anesthesia - combining the block of the infraorbital nerve (2% lidocaine without vasoconstrictor) and injection of 0.5% lidocaine in areas that remained sensitive.
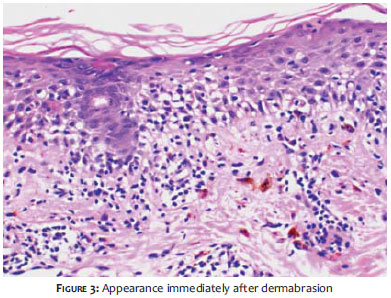
For the manual dermabrasion, sterile fine water sandpaper (granulation 100) was used until a pinpoint bleeding was formed and the pigment was visually completely removed. Sandpaper with 400 and 600 granulation was also used to achieve a more homogeneous and gradual appearance at the lesion's edges. The abrasion area was occluded with sterile transparent polyurethane film (Tegaderm®) for five days. Oral acyclovir was prophylactically administered for 2 days before and 3 days after the procedure. After the removal of the dressing (Figure 3) the patient used petrolatum jelly up until complete healing was achieved, thereafter using 0.05% clobetasol cream for 30 days, followed by 4% hydroquinone cream for 3 months. After that period, an ophthalmological evaluation and liver enzymes evaluation was carried out, and the authors introduced 400 mg/day hydroxychloroquine associated with 0.1% tacrolimus cream.
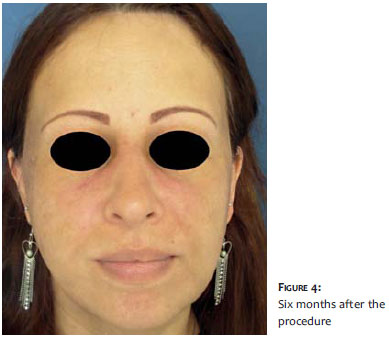
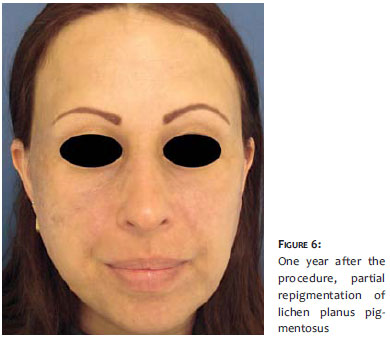
A satisfactory cosmetic outcome was achieved, and maintained - with mild local erythema - at 6 and 9 months after the procedure (Figures 4 and 5). Twelve months after the procedure, recurrence in small areas was observed, at which point new localized dermabrasion was indicated. The patient, however, chose to continue only with clinical treatment due to the fact that she was satisfied with her appearance (Figure 6).
Treatment of LPPig is difficult and the scarce literature on the topic describes resistance to topical corticosteroids and calcineurin inhibitors.4 There are reports of favorable outcomes with Nd:YAG laser,5 intense pulsed light6 and, despite the controversy, with topical tacrolimus.7
Dermabrasion is described for the treatment of LPPig and melasma, disorders that involve melanocyte activation and pigment incontinence.8 The proposed mechanism is the physical removal of the existing pigment through abrasion. Nevertheless there is a lack of case reports showing long-term follow up and results for this procedure.
The patient evaluated in the present study had almost complete improvement of the picture, with results being maintained during up to 1 year of follow-up, when small areas of recurrence could be noticed. The authors highlight the improvement in the patient's quality of life after one dermabrasession and that she has remained satisfied with the resulting aesthetic appearance up until the time the present paper was submitted, undergoing clinical treatment only (hydroxychloroquine and tacrolimus).
LPPig was recently linked to frontal fibrosing alopecia (FFA), and may precede its onset.9 This may suggest systemic involvement and the need for a broader approach of the pathology. The evaluated patient was diagnosed with AFF due to the loss of the eyebrows and slight recession of the frontal hairline. The biopsy of the scalp showed perifollicular lichenoid infiltrate, which justifies the authors' choice for the concomitant use of hydroxychloroquine.
In the present report the authors realized that dermabrasion was crucial for the removal of the facial pigment associated with LPPig. Despite the good development and the patient's satisfaction with the minimal recurrence in the 12-month followup, the authors deem further studies are necessary to determine the role and indications of dermabrasion in the treatment of LPpig.
1. Namazi MR. Lichen planus pigmentosus presenting as diffuse facial melanosis. J Drugs Dermatol. 2004;3(4):436-7.
2. Khanna N, Rasool S. Facial melanoses: Indian perspective. Indian J Dermatol Venereol Leprol. 2011;77(5): 552-64.
3. Kanwar AJ, Dogra S, Handa S, Parsad D, Radotra BD. A study of 124 Indian patients with lichen planus pigmentosus. Clin Exp Dermatol. 2003; 28(5):481-5.
4. Kim BS, Aum JA, Kim HS, Kim SJ, Kim MB, Oh CK, et al. Coexistence of classic lichen planus and lichen planus pigmentosus-inversus: resistant to both tacrolimus and clobetasol propionate ointments. J Eur Acad Dermatol Venereol. 2008;22(1):106-7.
5. Kim J-E, Won C-H, Chang S, Lee MW, Jee-Ho, Choi JH, et al. Linear lichen planus pigmentosus of the forehead treated by neodymium:yttriumaluminum-garnet laser and topical tacrolimus. J Dermatol. 2012;39(2):189-91.
6. Parada MB, Yarak S, Michalany NS. Tratamento do liquen plano pigmentoso com luz intensa pulsada. Surg Cosmet Dermatol. 2009;1(4):193-5.
7. Al Mutairi N, El-Khalawany M. Clinicopathological characteristics of lichen planus pigmentosus and its response to tacrolimus ointment: an open label, non-randomized, prospective study. J Eur Acad Dermatol Venereol. 2010; 24(5): 535-40.
8. Kunachak S, Leelaudomlipi P, Wongwaisayawan S. Dermabrasion: A Curative Treatment for Melasma. Aesth Plast Surg. 2001; 25(2):114-7.
9. Dovla NC. Frontal fibrosing alopecia and lichen planus pigmentosus: Is there a link? Br J Dermatol. 2013;168(2):439-42.
This study was conducted at the Hospital do Servidor Público Municipal de São Paulo (HSPM-SP), São Paulo (SP), Brazil.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}