


Ival Peres Rosa1; Sergio Henrique Hirata2; Mauro Yoshiaki Enokihara3; Ana Carolina Garcia Pozetti4; Caroline Benevides Farkas5; Anamaria da Silva Facina6
Keywords: HEMOSTASIS; HEMOSTASIS, SURGICAL; AMBULATORY SURGICAL PROCEDURES; SUTURES.
Hemostasis is a relevant and constant concern for all surgeons, with several hemostatic techniques having been described in the literature.1-3 Additionally, in recent years there has been an increase in the number of malignant skin tumors with surgical removal indication, particularly among immunocompromised patients.4 These lesions are often located in abundantly irrigated areas such as the scalp,5 can have large dimensions,6 and occur in patients with coagulation disorders7 or who are taking anticoagulants.
In order to assist in such situations, the authors describe a new prophylactic hemostasis technique that is useful for the resection of lesions of the type that present a risk of heavy bleeding. The authors propose performing a suture with separate, simple, closely spaced stitches, distributed in a way that externally surrounds the safety margin of the lesion to be excised. The authors have named this technique the hemostatic "enclosure".
Firstly, the lesion is marked with an adequate safety margin. Local anesthesia is then administered so that the anesthetic penetration occurs along a reference perimeter located 5 mm beyond the area intended for the "enclosure". If possible, a regional block anesthesia should be used in order to prevent local swelling. The "enclosure", which is located externally to the lesion's safety margin, begins then to be built. Interrupted simple stitches, are carried out side by side with enough space between them to prevent significant bleeding without disrupting local blood supply. In the scalp and with large lesions the "enclosure" should ideally employ 2-0 nylon threads with a 3.0 cm needle. The stitch must be passed with the needle perpendicular to the skin (in the scalp, the stitch should reach the galea aponeurotica), and the knot must be tight (in order to achieve this, the surgeon's assistant must seize it with a needle holder). The needle's length (3.0 cm) is more important than the thickness of the thread, since it must pass through the skin at all points of its thickness - which would not be possible with shorter needles. The needle passes deeply into the skin and emerges farther ahead, with a simple surgical knot then being performed. Continuous suture is not efficient due to the fact it provides lower pressure than that obtained with interrupted stitches.
Next the removal of the tumor is carried out, with hemostasis now made easier. In the case of an edge-to-edge closure of the surgical wound, the hemostatic "enclosure" can be left in place up until the removal of all stitches. When performing local flaps, the stitches of the "enclosure" that are located across the incision's path are removed; if there is bleeding, the "enclosure" can be extended to the region outside the flap's marking. This technique can also be performed after the surgery has begun; in cases of significant bleeding, the lesion's removal is interrupted and the hemostatic stitches are carried out, with the surgical time being subsequently resumed. The hemostatic sutures must remain in place for 2 or 3 weeks.
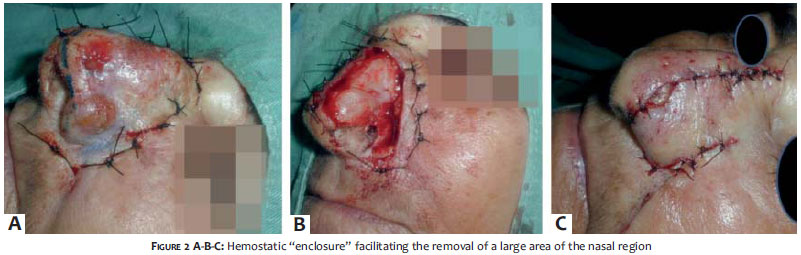
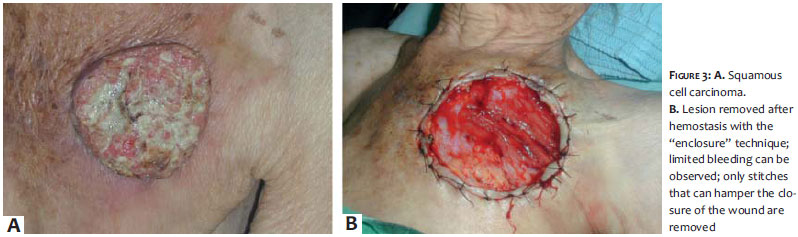
A significant reduction of bleeding can be observed during surgery. The presence of the hemostatic "enclosure" does not cause necrosis or damage to the borders. The use of this technique in grafts results – 7 days later – in a better appearance than those provided by other hemostatic techniques (Figures 1,2 and 3).
The hemostatic "enclosure" is indicated in all cases where there is presumption of a high risk of bleeding, such as large lesions on the scalp or nose. It can even be performed after surgery has started, in cases where there is more bleeding than expected. There are other ways to carry out hemostasis in the scalp, such as the use of saline with vasoconstrictor, manual compression, hemostatic forceps compressing vessels that bleed, knot of vessels, detachment beneath the galea and inserting a great amount of gauze.1, 2
With the implementation of the "enclosure" however, there is no need to control the amount of gauze used or the volume of injected anesthetic, which increases the safety of procedures.
A similar procedure was carried out in neurosurgery in which hemostasis was used with continuous stitches performed before the incision.8 The developers of the present technique propose carrying out the suture with interrupted simple stitches, distributed so as to build an enclosure that is located externally to the safety margin of the lesion to be excised. This procedure leads to a steep decrease in bleeding; nevertheless it does not cause it to cease. This is an advantage due to the fact that the enclosure's stitches can be left in place without risk of necrosis or damage to the skin. In addition, this technique can also be employed to remove small skin lesions - including scalp biopsies - with little bleeding and denouement. Cigna et al. described a method that employs the scissors' ring/hole, which can only be used for small lesions and occupies one of the surgeon's hands.9 Conversely, the method described in the present paper - after which profuse bleeding is in fact no longer observed - is effective for any size lesion and its use results in comfort and safety for the surgeon during the surgical procedure.
It is of paramount importance to understand that this procedure is carried out prior to the surgery itself and should not be mistaken for the "tobacco pouch" suture (marsupialization), which is performed after the removal of the lesion and whose function is to reduce the surgical wound.10 In the technique described by the present paper, the stitches are performed before the removal of the lesion.
The authors have observed a significant reduction in bleeding with the use of the "enclosure" technique. The stitches must remain in place for 2 or 3 weeks after the surgery - early removal can lead to significant bleeding, requiring new suture. This technique is not only useful for scalp, face, and trunk surgery, but also for body sites that may present significant bleeding, making it useful for preventing complications typical of other methods - such as granulomatous reactions, 1 or concern with patients fitted with pacemakers (in the case of use of electrosurgery).2 Another advantage of the "enclosure" technique is that it reduces the probability of ischemic complications resulting from hematomas due to their prophylaxis. The hemostatic "enclosure" method provides important innovation and assistance to dermatologic surgeons.
The hemostatic "enclosure" is a simple solution that increases the safety of the removal of skin lesions. This strategy allows removing large areas of the scalp, especially in transplanted patients, those on anticoagulant drugs, and those who have multiple confluent lesions in the same body region.
1. Howe N, Cherpelis B. Obtaining rapid and effective hemostasis: Part I. Update and review of topical hemostatic agents. J Am Acad Dermatol. 2013;69(5): 659.e1-659.e17.
2. Howe N, Cherpelis B. Obtaining rapid and effective hemostasis: Part II. Electrosurgery in patients with implantable cardiac devices. J Am Acad Dermatol. 2013;69(5): 677.
3. Glick JB, Kaur RR, Siegel D. Achieving hemostasis in dermatology-Part II: Topical hemostatic agents. Indian Dermatol Online J. 2013;4(3):172-6.
4. Ho WL, Murphy GM. Update on the pathogenesis of post-transplant skin cancer in renal transplant recipients. Br J Dermatol. 2008;158( 2):217-24.
5. Ulrich C, Schmook T, Sachse MM, Sterry W, Stockfleth E. Comparative epidemiology and pathogenic factors for nonmelanoma skin cancer in organ transplant patients. Dermatol Surg. 2004;30(4 Pt 2):622-7.
6. Panajotovic L, Dordevic B, Pavlovic MD. A giant primary cutaneous melanoma of the scalp--can it be that big? J Eur Acad Dermatol Venereol. 2007;21(10):1417-8.
7. Leonard AL, Hanke CW, Greist A. Perioperative management of von Willebrand disease in dermatologic surgery. Dermatol Surg. 2007;33(4):403-9.
8. Sakhai H. Hemostatic control of scalp incisions. Technical note. J Neurosurg. 1989;70(1):142.
9. Cigna E, Buccheri EM, Monarca C, Scuderi N. Hemostasis in skin surgery. Aesthetic Plast Surg. 2008;32(4):702.
10. Cohen PR, Martinelli PT, Schulze KE, Nelson BR. The purse-string suture revisited: a useful technique for the closure of cutaneous surgical wounds. Int J Dermatol. 2007;46( 4):341-7.
This study was conducted at the Universidade Federal de São Paulo (Unifesp) - São Paulo (SP), Brazil.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}