


Marisa Gonzaga da Cunha1; Ana Lúcia Gonzaga da Cunha2; Carlos A. Machado3
Keywords: SUBCUTANEOUS FAT; ADIPOSE TISSUE; SUBCUTANEOUS TISSUE.
Development of technologies for use with autologous adipose tissue has drawn attention to fat deposits, which represent an almost unlimited reservoir of stem cells accessible through minimally invasive procedures. Some of these deposits have until this point never been investigated. A growing number of experimental studies have demonstrated the potential of adipose stem cells l for neoangiogenesis and immunomodulatory action, as well as their use in treating ischemic and autoimmune diseases. The absence of scientific evidence corresponds to a hurdle in choosing a location for collecting samples.1
Moreover, the so called subcutaneous adipose tissue has recently been the object of growing interest since new surgical and non-surgical techniques have been proposed for their removal. These facts call for a deep knowledge of the embryological origin structure within the mesoderm, whose functions are storing energy, protecting against mechanical shock, enabling mobility in deeper structures, and acting as insulation. It also has a cosmetic effect, helping to shape the contours of the body.2
Adipose tissue has been empirically assumed by surgeons to be composed of two layers of fat (with differences between its lobules) divided by a membranous tissue layer. Its terminology varies according to atlases and textbooks, with the term fascia superficialis being the more frequently used (although improperly and inconsistently).3 Knowledge of the anatomy of superficial and deep fat tissue, called by some authors the superficial fascial system (SFS), allows for more well thought out and effective procedures to be conducted, though their terminology varies from author to author.4, 5 Based on studies of the anatomy of the abdominal wall, several authors have demonstrated that it is organized into the following layers, starting from the surface: skin (epidermis and dermis), superficial adipose or areolar tissue (SAT), a fibrous horizontal layer of connective tissue (membranous layer or fascia superficialis), deep adipose or lamellar tissue (DAT), deep fascia, and the abdominal wall muscles.3-5
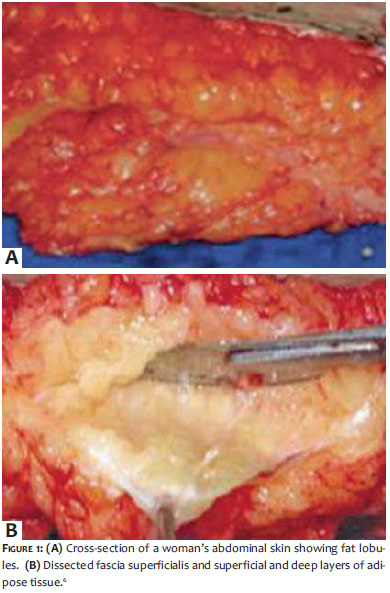
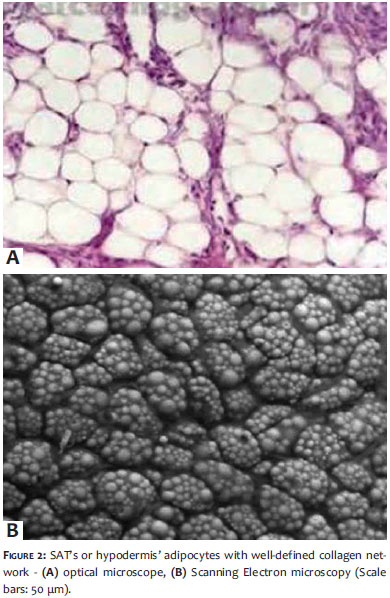
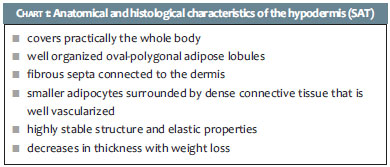
With the macroscopic dissection of the abdominal wall of 10 fresh cadavers of different physical structure (4 men and 6 women aged 48-93 years, mean age = 69 years), Lancerotto et al. identified a thin layer of adipose tissue underneath the dermis (Superficial Adipose Tissue) formed by fatty lobules and interspersed with fibrous septa, with a structure similar to that of honeycombs and which had a uniform distribution throughout the tissue. These septa (reticula cutis superficialis) were well defined and oriented perpendicularly towards the surface, and were strongly anchored to the dermis. (Figure 1)6 The fat lobules were organized into single or multiple layers, depending on the fat content of each individual's SAT thickness, and had no clear difference in the distribution both in the caudal and cranial directions, towards the thorax. It was possible to observe that the SAT was highly stable both in its structure and in its elastic properties, returning to its initial position after distention in the compression test.3 The SAT was histologically characterized by fibrous septa connecting the dermis with the fascia superficialis. These septa were composed of elastic and collagen fibers, which defined oval-polygonal lobules of fat cells,3 forming what Sbarbati called peri-adipocyte collagen network, with compartments well vascularized by capillaries.1 This structure plays an important role in preserving cellular integrity and can therefore influence the outcomes of autologous fat transplants (Figure 2).1
According to this description, it is possible to observe that this is the layer that is commonly defined as the hypodermis. Despite the clear anatomical distinction between dermis and hypodermis, both are structurally and functionally integrated via the network of vessels and nerves and via the presence of epidermal appendages.2 SAT or areolar tissue virtually covers the entire body in a layout with vertical compartments, distributed perpendicularly to the skin's more superficial layers. When there is weight gain, it increases in thickness.5, 6 With advancing age and in the presence of photodamage, it stretches and relaxes (like the dermis), resulting in the ptosis of soft tissue and in the formation of deformities due to pseudo deposits of fat.4
After removing the SAT, Lancerotto et al. observed a fibrous layer with a membranous appearance, apparently continuous and macroscopically well organized, with different thicknesses along the abdominal wall and thicker in the lower abdomen. This membrane merged medially with the linea alba, in the caudal direction with the inguinal ligament and with the bone prominences of the iliac crest; in the cranial direction it continued towards the thorax.3 Histologically, this membranous layer had multiple sub-layers of fibroelastic tissue consisting of collagen bands distributed in different directions, with intersection points between them and with fine irregular islands of adipose cells, located between the collagen fibers and with the appearance of lamellae.3, 5
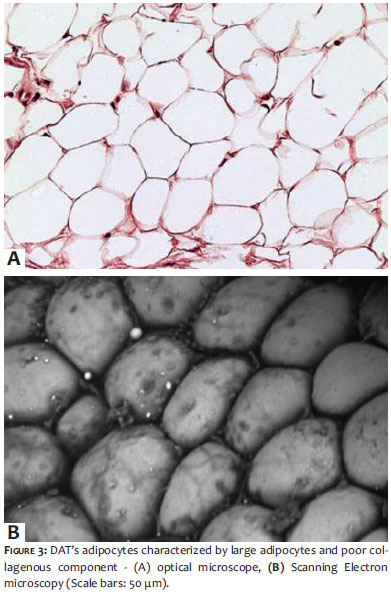
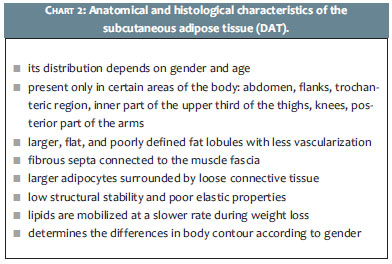
After removing the fibrous layer, Lancerotto et al. observed yet another layer of adipose tissue (deep adipose tissue - DAT), which Gasperoni et al. called the lamellar layer. It differs from SAT in appearance: it has larger, flattened, and less defined fat lobules, with less evident fibrous septa, and in general obliquely oriented and connected to the membranous layer of the deep fascia of the abdominal wall muscles.3 Sbarbati et al. describe this layer from the peri-adipocyte collagen network as incomplete, extremely fragile and finely adherent, with few vascular components, which apparently characterizes it as an area of high lipid deposition (Figure 3).1
The DAT layer or lamellar tissue overlays the deep fascia and the abdominal muscles, with significant variation in thickness. In the adhesion layers of the fibrous areas (inguinal ligament, linea alba and bone prominences) it is thinner due to the reduction of the fat component. Its thickness varied in fat content and mechanical strength among the studied individuals. The septa's oblique distribution, its limited elastic properties when stretched, and its low resistance under explain the sliding of this subcutaneous tissue over the deep fascia.3, 5
The DAT is present only in certain body sites: abdomen, flanks, trochanteric region, knees, back of the arms, and the upper third of the inner face of the thighs. In the instance of weight gain, it is responsible for localized deformations, when its thickness increases disproportionally more than that of the SAT.5
Lancerotto et al. also observed that SAT and DAT behave differently depending on the site of accumulation. In SAT, the thickness was almost uniform around the trunk. DAT tended to be thin in the anterior part, especially anterolaterally over the external oblique muscle, showing maximum thickness posterolaterally at the level of the flanks, where an accumulation was found.3 In addition, the thickness of both SAT and DAT varied among individuals: in the obese, the average thickness measured for SAT was 17.18 mm and for DAT 18.50 mm; in individuals with normal weight those values were 3.66 mm and 3.14 mm respectively. In both the obese and normal weight individuals, DAT's thickness increased progressively in the T10 - femoral head direction, while the thickness of SAT increased in the same direction only in the obese.3
In this manner, studies highlight that the distribution of the superficial and deep adipose tissue (SFS) varies in different body sites and from individual to individual, according to weight and gender. In certain sites it consists of several layers of fat and with obesity its distribution is almost indistinct. Anatomy differentiates body sites with both layers (SAT and DAT) and body regions that have SAT only. Inter-gender SFS variations entail differences in body contour and location of fat deposits. In the lower limbs of both genders, for instance, SAT was observed only in the anterior part of the thighs; in the inner, outer, and posterior parts of the medial portion of the thighs, in the ankles and in the anterior part of the arms. On the other hand, the trochanteric region of the female anatomy has a unique architecture, with the DAT's fibrous septa being firm and dense, and the fat being compact - resembling that of the SAT, in which lipids are mobilized at a slower rate and synthesized at a higher rate than in the abdominal region. 5 As a result, women have 51% of their DAT in the abdomen while men have 66%.7 In some body sites, SFS is firmly attached to the fascia or periosteum of the adjacent muscles, forming areas of adhesions, such as in the anterior and posterior middle line of the trunk, and in the inframammary and inguinal grooves and in the gluteus. In men, SFS is firmly adhered to the iliac crest region, while in women the zone of adherence is several centimeters below, determining the contour differences of the trunk region.5 For some authors, the polymorphism of the adipose tissue can determine different entities, depending on its location. Data from groups of patients with different ages indicate that the adipocytes' specialization and their metabolism can be partly related to the individual's life style. Weight loss is accompanied by an increase in the mobilization rate and a decrease in the fat synthesis rate in all tissues, although this change is more evident in abdominal fat than in the femoral fat.1 Regarding the resistance to insulin, the abdomen's DAT expresses a strong connection to the key aspects that define the insulin resistance syndrome, in a pattern similar to that observed for visceral adiposity,7 making it a major contributor to the metabolic consequences of obesity.8
In restorative therapies based on the implantation of cells, the structural morphology of the peri-adipocyte network and the presence of stem cell-rich microcirculation make SAT the optimal tissue for donor areas, particularly in places where the collagen network is thin, as in the trochanteric region and in the inner part of the knees.1
Traditional liposuction treats the deep adipose layer or DAT, avoiding the superficial layer, whose removal causes irregularities in the contour (Figure 4). On the other hand, the thickness of the SAT decreases with weight loss.5
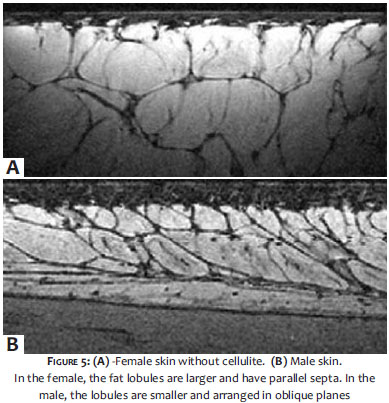
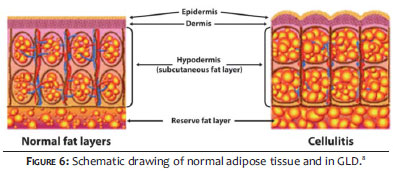
Cellulite or gynoid lipodystrophy (GLD) is a pathology specific to women due to the anatomical characteristics of SAT. In men, the fibrous septa are smaller and arranged in oblique planes with small fat lobules, whereas in women these lobules are larger and have parallel septa (Figure 5). These conditions exist from birth, however with the hormonal changes of puberty, greater storage of fat occurs along with interstitial fluid retention, and the fat lobules become enlarged due to the hypertrophy of the adipocytes, secondary to vascular alterations9,10 (Figure 6).8
In the female, the fat lobules are larger and have parallel septa. In the male, the lobules are smaller and arranged in oblique planes.
Adipose tissue should and needs to be divided into two distinct layers: hypodermis (SAT) and subcutaneous cellular tissue (DAT), for these layers have a completely different anatomy, histology, and metabolism (Charts 1 and 2).
The identification of novel aspects of the physiology of adipocytes and their established peculiarities are related not only to the skin's biology, but also become of paramount importance to better understand the dynamics of weight loss and localized fat deposition. When some researchers refer to the subcutaneous fat or adipose layer without precise observation of what is being anatomically and histologically described, it becomes impossible to discern which tissue the reference concerns.11
Further studies will undoubtedly reveal previously unknown concepts of the pathophysiology of adipocytes, and their ultrastructural and metabolic differences, which will lead to a better understanding of their behavior according to body site and consequently allowing a more precise determination of the best therapeutic approach.
1. Sbarbati A, Accorsi D, Benati D, Marchetti L, Orsini G, Rigotti G. et al. Subcutaneous adipose tissue classification. Eur J Histochem. 2010;54(4):226-30.
2. Chu, DH. Development and Structure of Skin. In: Wolff K, Goldsmith L, Katz S, Gilchrest BA, Gilchrest B, Paller A, et al. Editors. Fitzpatrick,s Dermatology in General Medicine, 7th ed. New York: The MacGraw-Hill Companies.Inc; 2008. p. 57-72.
3. Lancerotto L, Stecco C, Macchi V, Porzionato A, Stecco A, De Caro R. Layers of the abdominal wall: anatomical investigation of subcutaneous tissue and superficial fascia. Surg Radiol Anat. 2011;33(10):835-42.
4. Lookwood TE. Superficial Fascial System (SFS) of the trunk and extremities: a new concept. Plast Reconst Surg. 1991;87(6):1009-18.
5. Gasperoni G, Salgarello M. Rationale of Subdermal Superficial Liposuction related to the anatomy of subcutaneous fat and the Superficial Fascial System. Aesth Plast Surg. 1995;19(1):13-20.
6. Silva SL. Variações anatômicas do tecido celular subcutâneo pós-perda ponderal. Rev Bras Cir Plast. 2010;25(4):130-5.
7. Kelley DE, Thaete FL, Troost F, Huwe T, Goodpaster BH. Subdivisions of subcutaneous abdominal adipose tissue and insulin resistance. Am J Physiol Endocrinol Metab. 2000;278(5):E911-8.
8. Smith SR, Lovejoy JC, Greenway F, Ryan D, deJonge L, de la Bretonne J, et al. Contribuitions of total body fat, abdominal subcutaneous adipose tissue compartments, and visceral adipose tissue to the metabolic complications of obesity. Metabolism. 2001;50(4):425-35.
9. Paschoal LHC, Cunha MG, Ciporkin H. Fisiopatologia e Atualização Terapêutica da Lipodistrofia Ginóide - Celulite. 2ª ed. revisada e ampliada. São Paulo: Di Livros Editora Ltda; 2012. p.79-110.
10. Mirrashed F, Sharp JC, Krause V, Morgan J, Tomanek B. Pilot study of Dermal and Subcutaneous Fat Structures by MRI in Individuals that differ in Gender, BMI, and Cellulite Grading. Skin Res Technol. 2004;10(3):161-8.
11. Driskell RR, Jahoda CA, Chuong CM, Watt FM, Horsley V. Defining dermal adipose tissue. Exp. Dermatol. 2014;23(9):629-31.
This study was conducted at the Faculdade de Medicina do ABC (FMABC) - Santo André (SP), Brazil.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}