


Michael S. Christensen
Keywords: CELLULITE, RETINOL, CAFFEINE, DELIVERY SYSTEM
Cellulite is a colloquial term for deposits of fat and fibrous tissue that cause a dimpling appearance on the skin. The medical term for this condition is edematous fibrosclerotic panniculopathy.1 It was first described in the 17th century, and was simply attributed to an accumulation of fat. It was only recently that it was in fact recognized as a clinical entity.2
Cellulite occurs almost exclusively in post-pubertal women and is in fact present in some form in 80-95% of women. 3 Cellulite is much more complex than a simple accumulation of fat. The key factor is the presence of estrogen,4 which influences a vascular factor, and in turn controls the whole process. The sequence, which begins with a vascular component, is mediated by a specific factor. The final step in the process is the formation of dimpled islands of fat.
It is well known that estrogen plays an important role in the regulation of the skin's blood vessels, as evidenced by the flushed appearance and the telangiectasia seen with rosacea, as well as by the telangiectasias and severed vessels observed elsewhere in the skin, especially in the legs. With the increase in the number of vessels caused by estrogen, and due to the effects of gravity and pressure, vessel rupture occurs, resulting in blood release. This leads to the additional release of proteases, peptides and growth factors, resulting in swelling and inflammation, which triggers the healing process and subsequent fibrosis.
The cell that is primarily involved in wound healing is obviously the fibroblast, which promotes increased production of collagen and the altered synthesis of glycosaminoglycans. Due to the increase in peptides and growth factors, adipocytes increase in size and number, and become trapped in the regrowth of fibrous tissue.
In sum, the vessels weaken and rupture when under the influence of estrogen,5 the lipocytes accumulate and expand, the fibroblasts are activated and there is a remodeling of the subcutaneous space, which results in islands of fat surrounded by a newly synthesized fibrous network.
While it is a fact that almost all women will have cellulite at some point in their lives,2 this may occur to varying degrees, including only simple changes that do not have an impact on the personal appearance and may or may not develop into more serious alterations.
Based on many years of clinical observation, the following severity scale for cellulite was developed:
Grade I:The skin appears to be normal, however it displays an "orange peel" effect when pinched.
Grade II: The "orange peel" effect is visible even when the skin is not pinched.
Grade III: Horizontal depressions and dimples are visible on the skin, however there is no clear compartmentalization.
Grade IV: Clearly visible compartments, depressions, and dimples.
Grade V: Final stage of development; in addition to the compartmentalization and dimples, there is also skin over lapping.
There are many treatment modalities in use that are aimed at changing the appearance of cellulite. These include massage, endermologie, liposuction, laser, diet, and physical exercise. Since diet and physical exercise have proven ineffective, certain procedures - such as IPL (Intense Pulsed Light), vacuum massage systems, VelaSmoothTM, AlmaAccent®,6 RF System, Thermage® ThermaCoolTM,7 and Smooth ShapesTM8 100 among others - have become more prevalent. None of these methods has a significant amount of research ratifying its proposals. Invasive therapies - such as ultrasonic liposuction, smart lipo, subcision, and mesotherapy - have also not proven to be significantly beneficial in improving the appearance of cellulite, whether in the short, or long term.
Topical therapies with formulations containing methylxanthines - such as caffeine and theophylline, retinoids,9 and compounds that can affect blood circulation, such as Ginko Biloba and papain - were also tested and found minimally effective, perhaps due to their formulation.
An effective therapy should ideally act on all stages of the process that leads to cellulite formation. Furthermore, the results should be apparent to the physician and the patient, additional clinical damage must be avoided and, finally, the treatment should demonstrate efficacy and safety in appropriate clinical trials.
The objective of the trial described in the present paper was to evaluate the effects of a special topical formulation on the visible signs of cellulite, one that contains retinol, caffeine, vitamin C, and vitamin E in an optimized vehicle.
Effectiveness of the clinical trial described
The results of a clinical trial performed with a new topical treatment are presented below. Following the study protocol, a formulation containing the following ingredients was used: retinol (to improve the texture of the skin's surface and to stimulate glycosaminoglycans, collagen, and elastin), caffeine (to improve microcirculation and fat metabolism), vitamin C (to help in the synthesis of new collagen) combined with vitamin E (to provide antioxidant action). A patented system of topical delivery (AccudelTM)10 was used to improve the transmission of the ingredients to the skin. The test material (CELLURASE® Renewal Cream) was provided by resolutionMD, LLC.11
Accudel12 is a patented delivery system with a lipid matrix that stabilizes high concentrations of active ingredients, allowing fast and controllable transportation through the stratum corneum while minimizing systemic exposure. It is biocompatible, biodegradable, and non-immunogenic. This system is currently undergoing independent clinical trials for optimal topical delivery of ketoprofen for pain management.
The present study was designed with the purpose of determining the safety and beneficial effects of a formulation that uses the above-mentioned delivery system and ingredients to reduce the visible signs of cellulite. The study duration was 17 weeks. Twenty-five female patients aged between 25 and 60 years participated and were instructed to apply the test-cream every night before going to sleep. They were also instructed to apply a conventional moisturizer every morning after the removal of the test-cream.
The patients were evaluated after 2, 4, 8, 12, and 17 weeks of treatment. Evaluations consisted of digital photographs of the affected areas. The same precise body site was photographed in each evaluation, with carefully standardized lighting and positioning.
At each experimental point, the patients were asked to answer a questionnaire about product safety, aesthetic attributes and, especially, on their perception of the effectiveness of the treatment.
At the end of the study, two clinical evaluators rated the photographs independently using a 6-point subjective scale, where "0" corresponded to the absence of any signs of cellulite and "5" corresponded to severe cellulitis (Grade V in the described in severity scale).
A) Subjective evaluation (self-evaluation)
No undesirable effects were reported except for a slight dryness in the affected areas, which decreased with the use of a common moisturizer.
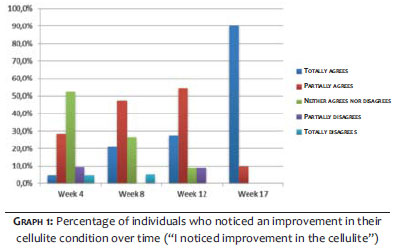
In general, efficacy was noticed from Week 4 and at the end of the study. Over 90% of participants noticed an improvement in the visible aspects of cellulite (Graph 1).
In Week 4, 33.4% of patients agreed with the statement "I have noticed improvement in the cellulite", with 4.8% strongly agreeing and 28.6% agreeing partially. Of the total group, 52.4% neither agreed nor disagreed and the 14.3% remaining did not notice improvement.
In Week 8, 68.5% of the patients agreed with the statement "I have noticed improvement in the cellulite", with 21.1% strongly agreeing and 47.4% partially agreeing. A total of 26.3% neither agreed nor disagreed and the 5.3% remaining did not notice improvement.
In Week 12, 81.8% of the patients agreed with the statement "I have noticed improvement in the cellulite", with 27.3% strongly agreeing and 54.5% agreeing partially. At this point in the study, 9.1% neither agreed nor disagreed and the remaining 9.1% did not notice improvement.
In Week 17, 100.0% of the patients agreed with the statement "I have noticed improvement in the cellulite", with 90.0% strongly agreeing and 10.0% agreeing partially.
B) Objective evaluation (performed by clinical evaluators)
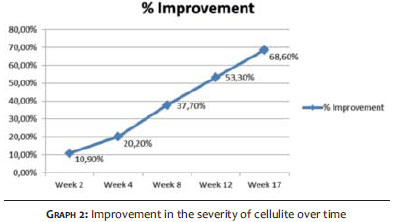
The two independent evaluators noticed a gradual overall improvement, reflected in the decreasing cellulite scores in each of the evaluation sessions. When the two independent assessments of the severity of the cellulite were normalized, a gradual improvement as compared to the baseline was observed regarding the appearance of the cellulite. (Graph 2), with a maximum value of 68.6% in Week 17, at the end of the study.
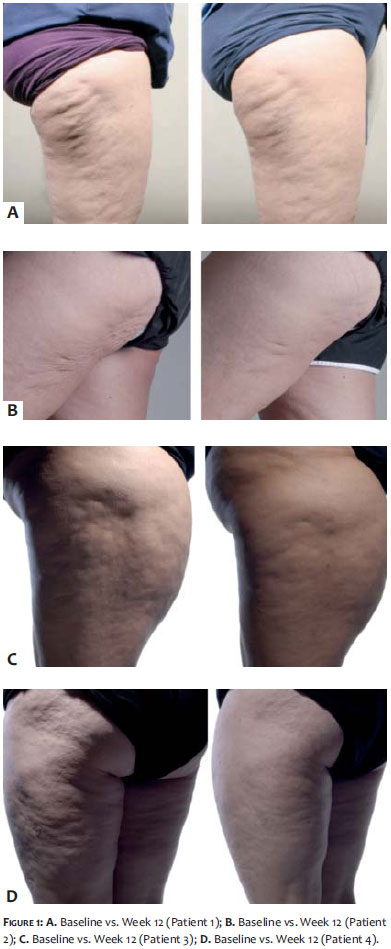
C) Photographic records
The following "before and after" photographs in pairs show the levels of improvement that were typically observed in the clinical trial. The baseline picture is always on the left hand side (Figure 1).
The evaluation of the various factors responsible for the development of cellulite allows for the conclusion that cellulite is a real clinical entity (and not simply an accumulation of fat), with a multifactorial cause, and that it should be treated as such.13
A substantial number of physical treatments for cellulite are commercially available, however the results are often unpredictable - and even if they are effective, the improvement does not last for long.
During the last twenty years, dozens of companies have sold cellulite-reducing creams,14 mainly based on the potential lipolytic activity of xanthines - caffeine in particular. None of these products has achieved significant marketplace success, probably due to their minimal effectiveness, even when retinol is added to the xanthines.
Many clinical studies have used a reduction in thigh circumference, or simply weight loss, as measures of efficacy. However, it is a well-known fact that body mass itself does not correlate to the presence or severity of cellulite. In the U.S. the Federal Trade Commission regulatory body has explicitly stated that claims of improvement to cellulite based on any of these measures are unacceptable, and severe fines have been levied to companies that make such claims.
Despite the apparent lack of commercial success with these ingredients (xanthines and retinol), there are reports of their beneficial effects, and, taking into account the changes in the subcutaneous tissue when cellulite is present, it can be expected that, if properly formulated, some retinol, xanthines, and vitamin combinations can reduce the external signs of cellulite.
The results obtained in the described clinical study indicate that topical therapy to treat the visible manifestations of cellulite can be effective when the appropriate ingredients are selected and incorporated into a topical delivery system designed to improve penetration into the skin. In addition, both patients and evaluators observed without difficulty an improvement in the cellulite, and remarkable improvement was observed after four weeks. Finally, the improvement was gradual, persisting for more than 17 weeks.
The author would like to thank resolutionMD, LLC for its support in supplying the tested formulation.
1. Avram MM. Cellulite: a review of its physiology and treatment. J Cosmet Laser Ther. 2004;6(4):181-5.
2. Numberger F. Muller G. So-called cellulite: an invented disease. J Dermatol Surg Oncol. 1998;4(3):221-9.
3. Pavicic T., Borella C, Kooting HC. Cellulite-the greatest skin problem in healthy people? An Approach. J Dtsch Dermatol Geo. 2006;4(10):861-70.
4. Wanner M, Avram M. An evidence-based assessment of treatments of cellulite. J Drugs Dermatol. 2008;7(4):341-5.
5. Mendelsohn ME, Kress RH. Estrogen and the blood vessel wall. Curr Opin Cardiol. 1999;9(5):619-26.
6. Alma Lasers [Internet]. Alma LasersTMUS, Buffalo Grove, IL 60084. [cited 2014 Dec 18]. Available from: http://www.almalasers.com/int/
7. Red Spot Interactive [Internet] Jupiter, FL 33458. [cited 2014 Dec 18]. Available from: http://www.redspotinteractive.com/
8. Kligman AM, Pagnoni A. Topical retinol improves cellulite. J Dermat Treatment. 1999;10(2):119-25.
9. PatentBuddy [Internet]. U.S. Patent No. 5,837,289 [cited 2014 Dec 08]. Available from: http://www.patentbuddy.com/Patent/5837289
10. Resolution MD [Internet]. Resolution MD, LLC, Henderson, NV 89074. [cited 2014 Dec 08]. Available from: http://www.trademarkia.com/resolutionmd-85740709.html
11. Imprimis Pharmaceuticals [Internet]. Imprimis Pharmaceuticals, Inc., San Diego, CA 9213. [cited 2014 Dec 08]. Avaiable from: http://imprimispharma.com/
12. Khan MH, Victor F, Rao B, Sadick NS. Treatment of cellulite: Part II. Advances and controversies. J Am Acad Dermatol. 2010:62(3):373-384.
13. Greenway FL, Bray GA, Heber D. Topical Fat Reduction. Obes Res. 1995;3 Suppl 4:561S-568S.
14. Dickinson B, Gora-Harper ML. Aminophylline for Cellulite Removal. Ann Pharmacother. 1996;30(3):292-3.
This study was performed at Springhouse Skin Research, PA - USA
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}