


Adilson Costa1,2; Samara Eberlin2; Adriana Chaib Ferreira Jorge3; José Alexandre Mendonça4; Ana Helena Kalies5; Caroline Silva Pereira6
Keywords: LASER; ABDOMINAL FAT; LYPOLISIS.
Obesity is a major health problem worldwide due to its high prevalence and morbidity. It is diagnosed using the body mass index (BMI), an anthropometric indicator.1
The layout of fat in the central region, determined by waist circumference characterizes visceral obesity and is associated with metabolic disorders2-4 such as hypertension, dyslipidemia, fibrinolysis, metabolic syndrome, chronic inflammatory process, atherosclerosis development acceleration, and may also result in cardiovascular or cerebrovascular events.1, 5
Laser therapy is a non-invasive procedure that can be used to reduce localized fat. It uses a wavelength specific to adipose cells while preserving adjacent structures such as nerves, blood vessels, and skin.6
In the present study, the authors used a low-frequency diode laser device (685nm, 40mW, 1.3watts, 120Joules / cm2 / 10 minutes) consisting of four plates with nine emission sources, which remained in contact with the skin during the session. Furthermore, the equipment has two lymphatic stimulation probes with a laser-emitting source at each, which are placed in the lymphatic drainage region of the treated area.
The present study is aimed at evaluating the reduction of abdominal fat in volunteers undergoing procedures with a low-frequency diode laser available on the Brazilian market.
A total of 60 healthy female volunteers aged between 18 and 50 years, skin phototypes I to III (Fitzpatrick classification), with 18.5 > BMI < 30.0 kg/m2, who had fat deposits in the abdomen were selected for evaluation. They were followed up for 31 days, after the study had received approval from the Institution's Research Ethics Committee.
The visits occurred on the days 0 (D0), 3 (D3), 7 (D7), 10 (D10), 14 (D14), 17 (D17), 21 (D21), 24 (D24), 28 (D28), and 31 (D31). The following assessments were performed at each visit: evaluation of waist circumference (both before and after the laser application) in three predefined areas: upper (4.0 cm above the navel), median (on the navel) and lower (4.00 cm below the navel); measurement of the height of the navel from the floor (the patients were barefoot); application of a questionnaire to assess degree of pain (0-10 scale). In addition to these procedures, a satisfaction questionnaire (0-10 scale) was applied, the weight was measured, and the BMI was calculated at D0, D14, and D31 visits.
In each of these 10 visits, the volunteers underwent an application of a low-frequency diode laser (i-Lipo, Chromogenex Comércio, Importação, Exportação de Produtos Médicos Ltda. ANVISA Class II. 80332760006; 685nm, 40mW, 1.3watts, 120Joules/cm2/10 minutes) for 20 minutes. The plates were placed on the skin in the region to be treated; two emission probes with the same wavelength were placed on the point of lymphatic drainage in the area.
As directed by the manufacturer the volunteers were asked to perform 30 minutes of aerobic activities during the subsequent 60 minutes. The clinical efficacy assessment was carried out by analysis of photographs and ultrasound examinations aimed at comparing the thicknesses of the dermis.
The descriptive statistics and the evaluation questionnaires allowed to draw conclusions about the participants' demographic profile. In order to analyze the changes between assessments, the ANOVA for repeated measurements, followed by the contrast profile test were used to compare the results of the physical measurements (waist circumference, weight, BMI, ultrasound data). Data were processed into ranks due to the lack of normal distribution. The significance level was set at 5.0%. The SAS (version 9.3) software was used to perform the analyses.
Fifty volunteers (from a total of 60) completed the study. Of these, 11 (22.0%) had skin phototype II, and 39 (78.00%) had phototype III, with a mean age of 39 years (range = 18 to 51 years).
The results of the evaluation of satisfaction with the laser application, immediately after each session was finished, were positive throughout the study period (D0 = 8.50; D14 = 8.62; D31 = 9.26), without statistically significant variation in the results in the comparison between visits (p = 0.4771; Table 1). Regarding the pain scale, 50 participants reported Grade 1 in all visits - except for one who reported Grade 2 pain on D0, progressing to Grade 1 in the other assessments (Table 2).
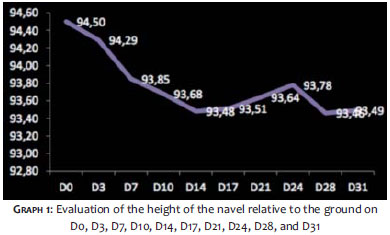
The variables weight (p = 0.9427; Table 3) and BMI (p = 0.9016; Table 4) did not present statistically significant reduction in the comparison between the visits and the baseline. Regarding the measurement of the navel's height, there was a statistically significant reduction in the comparative results between the visits and the baseline (D0 = 94.50 cm; D31 = 93.49cm; D0 vs. D31: 1.07% reduction; p <0.0001) (Graph 1).
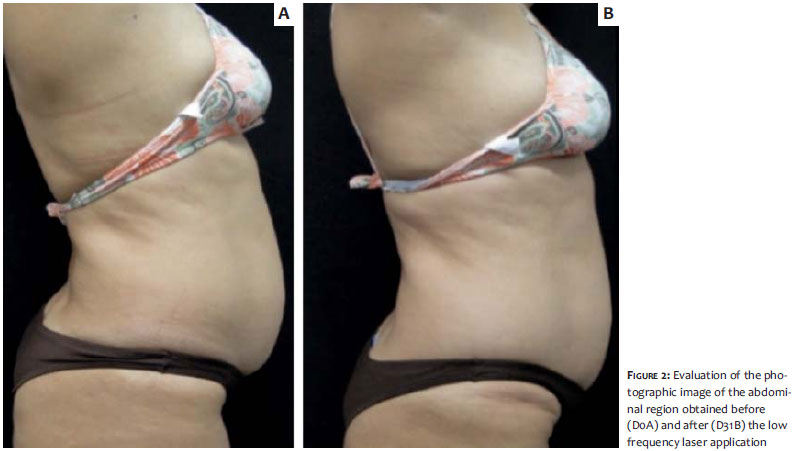
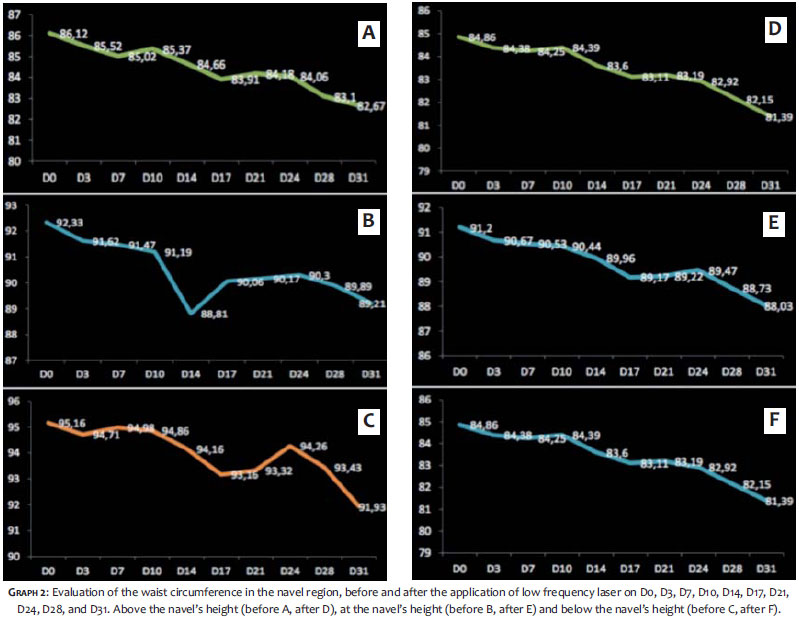
As depicted in Figure 2, the diode laser therapy decreased by 4% (p <0.0001; Graph 2A); 3.3% (p = 0.0026; Graph 2B) and 3.7% (p <0.0001; Graph 2C), respectively in the upper, median, and lower waist circumferences when measured before the laser session. Nevertheless, an interesting fact is that when evaluating these measurements after the completion of the session, it was observed that for the upper, median, and lower circumferential measurements, the reduction was 4.0% (Graph 2B), 3.47% (Graph 2D), and 4.0% (Graph 2F), respectively (all with p <0.0001). When carrying out the before and after analysis, the circumferential measurements were always lower after the application, suggesting that the technology had an immediate effect on the decrease of the measurements.
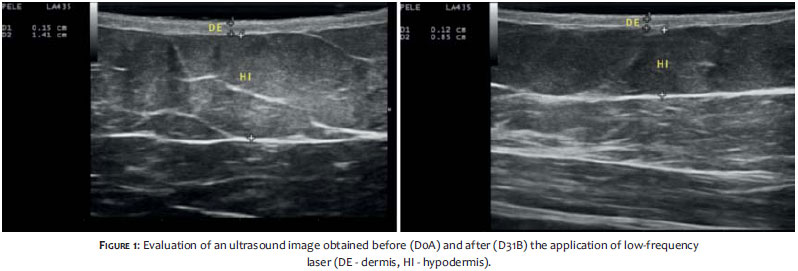
The analysis of the ultrasound data also showed a significant reduction from the baseline measurements (D1), and those taken on D31 of the dermis and hypodermis (18.75% and 20.45%, respectively; p <0.0003 for the dermis and p = 0.0229 for the hypodermis) (Tables 5 and 6, respectively; Figure 1). The reduction of abdominal thickness can also be visualized through the photographs taken on D0 and D31 (Figure 2).
Central or visceral obesity is closely related to potentially life-threatening cardiovascular complications.1,5 Behavioral measures based on lifestyle changes, weight loss, physical activity, and cessation of harmful habits (smoking, alcohol use) are key for primary and secondary prophylaxis of these events.7
Jackson et al. published the benefits of using a diverse, low frequency diode laser device (532nm) to treat gynoid lipodystrophy in 34 volunteers (three 30-minute applications per week, in the region of the thighs and buttocks). A group with the same number of volunteers underwent a "placebo" treatment (without emission of energy).8 For these authors, 19/34 (55.8%) of the volunteers had a statistical reduction of one level in the Nurnberger-Muller scale, as compared with 3/34 (8.8%) from the untreated group. The treated group also saw an improvement in their body circumference, weight, and body mass index. Six weeks after the end of the study, four volunteers from the treated group still had favorable results, a fact that was not observed in the untreated group.
Although there was no reduction in weight and body mass index in the volunteers of the present study, the low frequency diode laser therapy showed significant results for the reduction of localized fat, which were demonstrated through the reductions in the abdominal circumference measurements, the change in the height of the navel, and the ultrasound scale of the hypodermis. Also, there was dermal compression by the ultrasound. These results are unprecedented in the literature regarding the technological device studied.
The results obtained demonstrate the potential of the low potency diode laser to become an auxiliary technology in the reduction of abdominal fat.
1. World Health Organization. Obesity: preventing and managing the global epidemic. Report of a WHO consultation on obesity. Geneva: World Health Organization; 1998.
2. Organização Mundial da Saúde. Physical status: the use and interpretation of anthropometry. Geneva; WHO; 1995.
3. Cabrera MAS, Jacob Filho W. Obesidade em idosos: prevalência, distribuição e associação com hábitos e comorbidades. Arq Bras Endocrinol Metab. 2001;45(5):494-501.
4. Martins IS, Marinho SP. O potencial diagnóstico dos indicadores da obesidade centralizada. Rev Saúde Pública. 2003;37(6):760-7.
5. Janssen I, Heymsfield SB, Allison DB, Kotler DP, Ross R. Body mass index and waistcircumference independently contribute to the prediction of non-abdominal, abdominalsubcutaneous and visceral fat. Am J Clin Nutr. 2002;75(4):683-8.
6. Neira R, Arroyave J, Ramirez H, Ortiz CL, Solarte E, Sequeda F, et al. Fat liquefaction: Effect of low level laser energy on adipose tissue. Plast Reconstr Surg. 2002;110(3): 912-22.
7. World Health Organization / Food and Agriculture Organization. Diet, nutrition and the prevention of chronic diseases. Geneva: World Health Organization; 2003. (TechnicalReport Series, 916).
8. Jackson RF, Roche GC, Shanks SC. A Double-Blind, Placebo-Controlled Randomized Trial Evaluating the Ability of Low-Level Laser Therapy to Improve the Appearance of Cellulite. Lasers Surg Med. 2013;45(3):141-7.
This study was conducted at Kolderma Instituto de Pesquisa Clínica Eireli and at the Dermatology Department of the Pontifícia Universidade Católica de Campinas - Campinas (SP), Brazil.
 All content the journal, except where identified, is under a Creative Commons Attribution-NonCommercial 4.0 International license - ISSN-e 1984-8773
All content the journal, except where identified, is under a Creative Commons Attribution-NonCommercial 4.0 International license - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}