


Ana Carolina Souza Porto1; Sadamitsu Nakandakari2; Cleverson Teixeira Soares3
Keywords: FIBROMA; NEOPLASM; NAIL DISEASES.
Superficial acral fibromyxoma (SAF) was first described in 2001 by Fetsch et al. in a series of 37 cases. 1 Since then approximately 100 cases have been reported in the literature. 2 Yet this neoplasia is still poorly recognized by pathologists and dermatopathologists, partly due to its relatively uncommon occurrence, and partly because it has only recently been described. 3 It is a benign, slow-growing mesenchymal tumor, with no reports of malignant transformation or metastasis. The SAF has a clear tendency to involve the nail and periungual regions of the hands and feet. Middle-aged men are more frequently affected, with previously published case series suggesting that toes are more affected than fingers. 4 The usual treatment is complete surgical resection of the lesion, with a few cases of recurrence having been associated with incomplete resection. 2
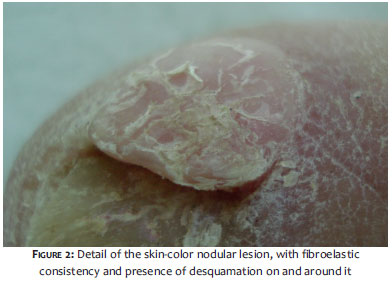
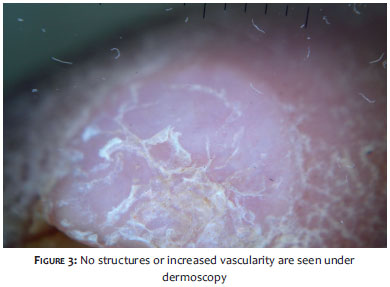
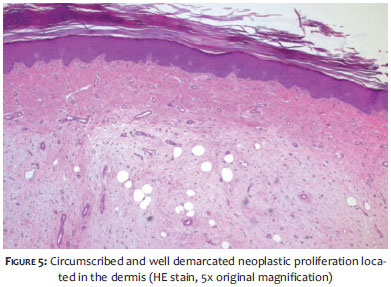
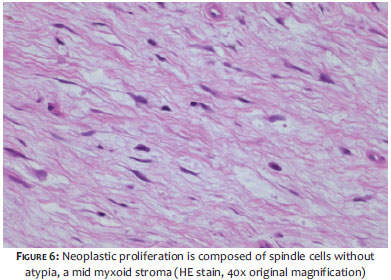
A 75-year-old mulatto female patient sought care complaining of a "callus" in the foot for three years. She denied pain or trauma preceding the onset of the lesion. The physical examination showed nodules of approximately 1 cm, with a color similar to that of the skin, fibroelastic consistency, and slight scaling located in the medial nail fold of the left big toe. It also presented with constitutional melanonychia and desquamation around the nail of that toe (Figures1 and 2). Dermoscopy showed intense subungual hyperkeratosis without the presence of specific structures and no vascularization (Figures 3 and 4). The patient underwent an excisional biopsy with the histology revealing a dermal mesenchymal lesion composed of stellate or spindle-shaped fibroblasts without atypia, permeated by capillaries a mid the myxoid matrix. The immunohistochemical analysis revealed diffuse expression of CD34, focal expression of CD99 and EMA with an absence of expression of the S-100 protein, or desmin and actin of the smooth muscle tissue. The clinical pathological features associated with the immunohistochemical profile defined the diagnosis of superficial acral fibromyxoma (Figures 5 and 6). The patient is still undergoing follow-up without signs of recurrence.
Superficial acral fibromyxoma affects more men than women (2:1), typically between the ages of 14- and 75-years-old, with a mean age at diagnosis of 43 years. 2,5 The SAF tends to present as a slow growing, firm mass or nodule, almost always located in the toes and fingers. 3 However, it can less commonly affect palms, heels, ankles, and thighs. 4 The nail is involved in 50% of cases, with hyperkeratosis or onychomycosis. A history of trauma preceding the appearance of the lesion is rare. 6 The SAF is characterized by being painless, a fact that explains the delay of patients in seeking medical care. 1 It is histologically characterized by a well-circumscribed dermal or subcutaneous tumor with increased vascularization, constituted by fusiform or stellate cells embedded in alternating areas of fibrous and myxoid stroma. The presence of significant nuclear atypia is rare and although it has been described in isolated cases, it causes concerns about the biological potential of the tumor. None of the tumors examined showed frank sarcomatous change, and no case of malignant transformation has been described in the literature. 2,3 The SAF is immunopositive for CD34, CD 99, and EMA, and negative for cytokeratin, melanocytic markers, SMA, and desmin. 3 The differential diagnosis of SAF should include consideration of ungual/periungual fibroma, acquired digital fibrokeratoma, low-grade fibromyxoid sarcoma, dermatofibroma, superficial angiomyxoma and myxoid neurofibroma.
The treatment of choice for SAF is surgical resection with free margins. Periodic monitoring is recommended after excision, and recurrence rates are estimated in the range of 10-24%. 6 Recurrence has been associated with incomplete resection. 2,5 The patient described showed no signs of recurrence of the lesion during a long follow-up. Although rare, SAF should be included in the differential diagnosis of tumors involving fingers and toes. 5
1. Fetsch JF, Laskin WB, Miettinen M. Superficial acral fibromyxoma: a clinicopathologic and immunohistochemical analysis of 37 cases of a distinctive soft tissue tumor with a predilection for the fingers and toes. Hum Pathol. 2001;32(7):704-14.
2. Messeguer F, Nagore E, Agustí-Mejias A, Traves V. Superficial acral fibromyxoma: a CD34+ periungual tumor. Actas Dermosifiliogr. 2012;103(1):67-9.
3. Prescott RJ, Husain EA, Abdellaoui A, Al-Mahmoud RM, Khan M, Salman WD, et al., Superficial acral fibromyxoma: a clinicopathological study of new 41 cases from the U.K.: should myxoma (NOS) and fibroma (NOS) continue as part of 21st-century reporting?. Br J Dermatol. 2008;159(6):1315-21.
4. Hollmann TJ, Bovée JV, Fletcher CD. Digital Fibromyxoma (Superficial Acral Fibromyxoma): A Detailed Characterization of 124 Cases. Am J Surg Pathol. 2012;36(6):789-98.
5. Ashby-Richardson H, Rogers GS, Stadecker MJ. Superficial acral fibromyxoma: an overview. Arch Pathol Lab Med. 2011;135(8):1064-6.
6. Wei C1, Fleegler EJ. Superficial acral fibromyxoma of the thumb. Eplasty. 2013: ic 13.
The present study was carried out at the Instituto Lauro de Souza Lima (ILSL) - Bauru (SP), Brazil.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}