


Fabiane Andrade Mulinari Brenner1; Lismary Aparecida de Forville Mesquita2; Jonathan Barbieri Hauschild3; Amanda Guiomar Simeão3
Keywords: HYPERPIGMENTATION; CERATOSIS; MINOCYCLINE.
Confluent reticulate papillomatosis (CRP) was described by French dermatologists Gougerot and Carteaud in1927. Its etiology is unclear. Among hypotheses for the development of CRP are a disorder of keratinization and/or an abnormal response to microorganisms of the skin's biota. Lipophilic yeasts of the Malassezia genus are among the main suspects of involvement. 1,2 The disease is most common among women aged 10 to 35 years, with higher skin phototypes (IV to VI).
It is clinically characterized by verrucous, brownish papules approximately 5mm in diameter, which are confluent in the center and have a peripheral reticulate pattern. The most affected body sites are: the trunk, intermammary region, and dorsal and epigastric areas. It is possible for the lesions to extend to the shoulders, neck, and pubic region. Occasionally, the extremities can be affected. The palmar and plantar regions and mucous membranes are usually spared. There may be pruritus, however the greatest discomfort is of an aesthetic nature. 3,4
The three elements of CRP diagnosis are: 1) Clinical - papillomatous lesions of light-brown color, with confluent center and reticulate in the periphery; 2) Microbiological - direct-examination and biopsy without evidence of fungal elements; and 3) Histological - hyperkeratosis, papillomatosis, acanthosis, and occasional hypogranulosis, and sparse superficial inflammatory perivascular infiltrate. 5 Histology is nonspecific, and skin biopsy unnecessary in most cases. The most frequent findings are: hyperkeratosis and papillomatosis, thinning of the stratum granulosum and interpapillary focal acanthosis. Sometimes the vessels of the papillary dermis may show ectasia and perivascular lymphocytic inflammatory infiltrate. Basal layer hyperpigmentation can occur without alteration in the number of melanocytes. 6
The main differential diagnosis is carried out with tinea versicolor (TV), which is more common than CRP. While CRP may not be as rare as reported in the literature, it is prone to under diagnosis -especially because some cases may respond to the usual therapy with TV. However, CRP should be suspected whenever a TV diagnosis does not improve after being treated with an antifungal. There is no standard therapy and several agents have been used with varying results. 7 Benzoyl peroxide, ammonium lactate, urea, tretinoin, clindamycin, sodium hyposulphite, and vitamin D analogues have been described with topical use. Among systemic treatments, minocycline, etretinate, and isotretinoin are among the most used. 8 The use of topical or systemic antifungals can be considered, especially when there is doubt about the differential diagnosis with TV. Although several drugs have been used with relative success, there is no uniformly effective agent due to the fact that it is a condition whose etiology is unknown. However, with the two present case reports it was possible to analyze the effectiveness of CRP treatment using minocycline, with a sustained therapeutic response, and therefore to help patients who have this diagnosis by providing a proven treatment option
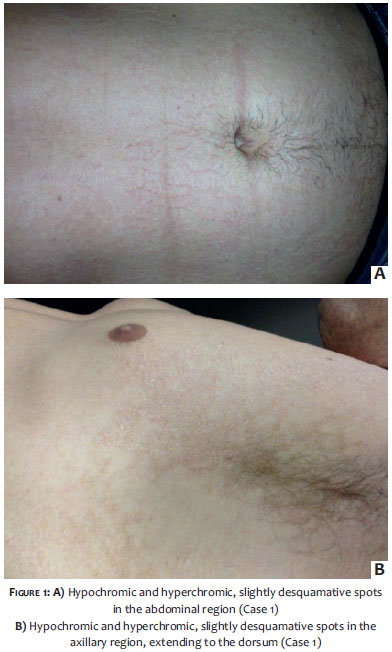
Case 1: A 24-year-old Caucasian male patient, from the city of Curitiba (Paraná State, Brazil) had slightly scaly, hypo- and hyperchromic spots for four years in the abdominal, axillary, and dorsal regions (Figure 1). He underwent various topical and systemic treatments for tinea versicolor, with partial response and lesion recurrence.
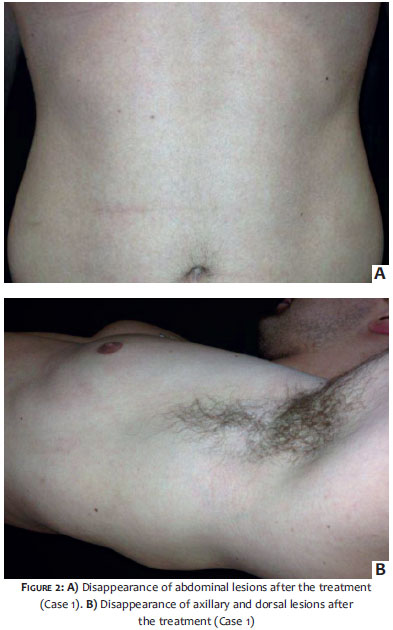
Direct mycological examination and a culture of fungi taken from material swabbed from the anterior thorax were negative. The suspicion of CRP arose and minocycline was initiated at 100mg/day for eight weeks. The lesions disappeared at the end of treatment (Figure 2), and there was no recurrence after 12 months.
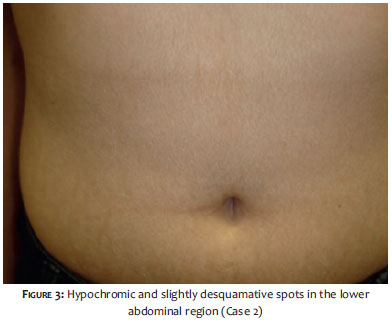
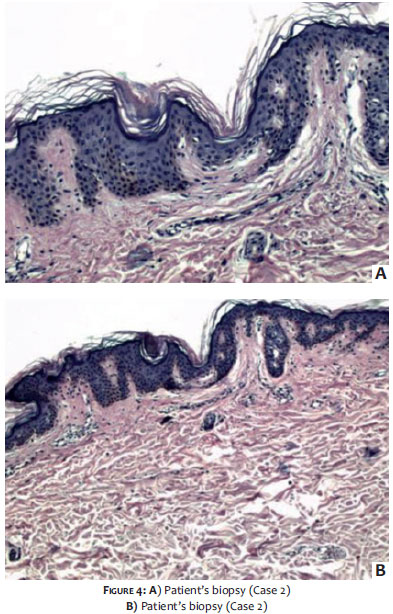
Case 2: A 20-year-old Caucasian female patient complained of scaly and hypochromic spots that she had in the abdominal region and on her back for three years (Figure 3). She had used ammonium lactate, with improvement and recurrence. Medications for tinea versicolor were also attempted without improvement. A biopsy was carried out (Figure 4), and fungi were not observed. The suspicion of CRP arose and minocycline was introduced at 100mg/day, for ten weeks. The lesions disappeared at the end of treatment and there was no recurrence for 36 months (Figure 5).
The emergence of CRP is generally more common in young adults, with an average patient age of 21 years. 6 Aligned with the data in the literature, the average age of onset of the dermatoses in both cases in this study was 18.5 years. Both patients had seborrheic skin, aggravated by excessive sweating during physical activity while wearing clothes without absorption capacity. The same characteristics had been verified in a previously reported case, 6 in which the presence of the symptoms were also correlated with sweat.
Most cases that have been described are of sporadic CRP, however there are some reports of the occurrence in two or more members of the same family. 3 In line with most cases reported in the literature, the two studied patients denied similar lesions in their families. Although records suggest a higher incidence of CRP in dark-skinned people, the patients studied in the present article were fair-skinned.
Regarding the treatment, in the studied cases there was a favorable response to the administration of minocycline at 100mg/day during a variable period of 8 to 10 weeks, with no recurrence after 12 months. That fact corroborated other reports, 7-10 leading the authors to conclude that this is a safe and effective alternative.
1. Dias MFRG, Azulay RD. Ceratoses foliculares. In: Azulay RD, Azulay DR, editores. Dermatologia. 3 ed. Rio de Janeiro: Guanabara Koogan; 2004. p.452-5.
2. DiGiovana JJ. Ichthyosiform dermatoses. In: Freedberg IM, Eizen AZ, Wollf K, Austin KF, Goldsmith LA, Kats S, et al. Dermatology in General Medicine. 6 ed. New York: Mc Graw-Hill; 1999.p.481-505.
3. Schwartzberg JB, Schwartzberg HA. Response of Confluent and Reticulate Papillomatosis of Gougerot and Carteaud to Topical Tretinoin. Cutis 2000;66(4):291-3.
4. Berger CM. Clinical Pathologic Challenge: confluent and reticulated papillomatosis of Gougerot and Carteaud. Am J Dermatopathol. 2003;25(1):82-5.
5. Lee MW. Syringoma resembling confluent and reticulated papillomatosis of Gougerot & Carteaud. Cutis.1998;61(4):227-8.
6. Carneiro FAR, Dias LM, Silva ACMS. Papilomatose confluente e reticulada de Gougerot-Carteaud: relato de caso. Rev Paran Med. 2008;.22(1):63-8.
7. Orrego GV, Jaimes AFT, Bisso KEC, García CJ. Papilomatosis reticulada y confluente (síndrome de GougerotCarteaud): reporte de tres casos tratados con minociclina. Rev Soc Peruana de Dermatología. 2011;21(4):158-62.
8. Rodríguez-Carreón AA, Arenas-Guzmán R, Fonte-Avalos V, Gutiérrez-Mendoza D, Vega-Memije ME, Domínguez-Cherit J. Papilomatosis reticulada y confluente de Gougerot-Carteaud. Un caso con excelente respuesta a minociclina. Gac Méd Méx. 2008;144(1):67-70.
9. Tseng HW, Tseng HH, Wu CS. Confluent and reticulate papillomatosis treated with minocycline and tazarotene. Cutis. 2013;91(4):194-7.
10. Hudacek KD, Haque MS, Hochberg AL, Cusack CA, Lee Chung C. An Unusual Variant of Confluent and Reticulated Papillomatosis Masquerading as Tinea Versicolor. Arch Dermatol. 2012;148(4):505-8.
The present study was carried out at Centro Especializado da Pele (Cepelle) - Curitiba (PR), Brazil.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}