


Lidicie Natalia Braga de Oliveira1; Fernanda Tolstoy2; Dolival Lobão3
Keywords: BASAL CELL NEVUS SYNDROME; CARCINOMA, BASAL CELL; EPIDERMAL CYST
Gorlin-Goltz syndrome or basal cell nevus syndrome is a dominant autosomal disorder characterized by early onset of basal cell tumors, and may also present other phenotypic abnormalities, for instance palmoplantar punctate pittings, odontogenic mandible cysts, and abnormalities in the ribs.1
Basal cell carcinoma (BCC) cutaneous lesions, as well as other skin alterations, may be present from birth or develop during childhood, though their occurrence is more frequent between puberty and 35 years of age. The number and type of lesions can vary within the same family, and there are marked differences in clinical manifestation between individuals from dark and light skinned populations. 1,2
In many cases, the BCC cutaneous lesions can resemble nevi or fibromas, and speculation about their actual diagnosis is sometimes possible only with the addition of thorough clinical and family histories, as well as other clinical and physical aspects associated with the patient.
A 39-year-old Caucasian male patient, who was born and brought up in the northeast Brazilian State of Bahia and worked as a farmer, was referred to the Brazilian National Cancer Institute (INCA). He complained about the emergence of diffuse tumor lesions throughout the body, which had grown progressively for nearly 20 years. The patient reported prior excision of some lesions and denied both similar family history or other comorbidities.
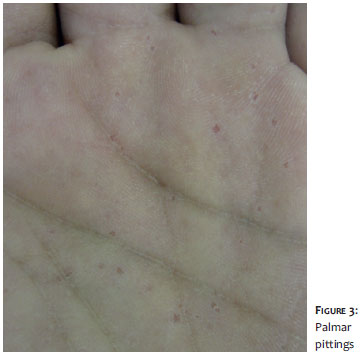
The dermatological examination showed multiple tumor lesions on the face (Figure 1), trunk, and upper limbs (some of them ulcerated, suggestive of BCC), in addition to diffuse nodular cystic lesions on the dorsum and upper limbs (Figure 2: A, B and C). He also had a large number of palmar pittings. There was an absence of cognitive deficits or neurologic alterations (Figure 3).
During the investigation, a skull and face tomography showed cutaneous thickening of an exophytic aspect, with infiltration of the lacrimal fossae, malar region, and upper lip; ectasia of the supratentorial ventricular system; extensive calcification of the tentorium and falx cerebri; multiple lytic expansive formations, which were sparse in the maxilla and mandible, consistent with keratocysts and sessile osteoma in the anterior wall of the right frontal sinus.
Also, biopsies of the tumor and nodular cystic lesions were carried out with a histological outcome compatible with BCC and epidermal cyst, respectively. In light of the clinical, radiological, and histological findings, it was concluded that this was Gorlin-Goltz syndrome with exuberant clinical findings.
The basal cell nevus syndrome (BCNS), or Gorlin-Goltz syndrome, is inherited through dominant autosomal transmission, has high penetrance and variable expressivity, and is characterized by the mutation of the PTCH1 gene, which is a tumor suppressor. Its estimated prevalence ranges from 1/57,000 to 1/256,000 individuals and is more common in Caucasians. 2
The PTCH1 gene, mapped on chromosome 9 (q22. 3q31), plays a fundamental role in the control of growth and development of normal tissues. The gene's product is a protein transmembrane component (Ptc, from patched), which in the presence of the Sonic Hedgehog protein, activates another protein transmembrane component (Smo, from smoothened). The activation of the latter promotes the transcription - in certain cells -of genes that encode signaling proteins belonging to the TGF-beta family (Transforming Growth Factor-beta) and WNT (wingless-type MMTV integration site), facilitating the cell decrease and differentiation processes. 3,4
The characteristic signs and symptoms of the syndrome were recorded by Jarish in 1894. In 1960, Gorlin and Goltz described them as a triad, including the BCC and numerous keratocysts in the mandibles and skeletal abnormalities. Their work on this description is how the term Gorlin-Goltz syndrome was coined. 5
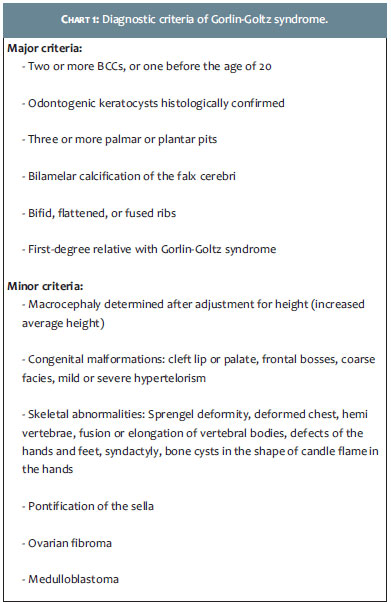
The diagnostic criteria for the basal cell nevus syndrome, which were established by Evans et al. and modified by Kimonis et al. in 1997, are listed in Chart 1, with the diagnosis being confirmed when two major criteria, or one major and two minor criteria, are present. 6
In the reported clinical case, the patient had three major criteria (multiple BCCs, palmar pittings, and calcification of the falx cerebri). The odontogenic keratocysts did not have a histological confirmation.
Epidermal cysts are infrequent findings in BCNS, however there are a few cases reporting this manifestation. 7 The mean age for the onset of BCC varies between 20 and 21 years. Variable in number - from just several to hundreds -they can occur in any area of the body, whether or not there has been exposure to solar radiation. 8 BCCs also have variable clinical behavior, and can be very aggressive from the onset, especially on the face. The predisposition to the development of BCC appears to be caused by the fact that the cells affected by the mutation are more susceptible to sunlight, due to the mechanism of DNA repair altered by the mutation. 9
The mandible keratocysts occur in 75% of patients and have a recurrence rate of 60%. Seventy percent of patients had hypertelorism, which sometimes is associated with the widening of the nasal root. Approximately 80% have palmar or plantar pittings. 6
Therapy aims at completely excising the tumors, especially BCCs and odontogenic keratocysts. Since the facilitation of the Sonic Hedgehog's signaling pathway is permissive for tumor development, the specific pharmacological treatment (Vismodegib) aimed at inhibiting that pathway is likely to be the future treatment strategy. 10
In the case described, the therapeutic approach was not implemented in the dermatological service, due to the fact that the patient was transferred to his city of origin for treatment.
The diagnosis and treatment of Gorlin-Goltz syndrome require a multidisciplinary approach by dermatologists, plastic surgeons, head and neck surgeons, neurologists and neurosurgeons. Genetic counseling and screening of family members are essential. Awareness of the extreme sensitivity of such patients regarding ionizing radiation in necessary, with the presence of the potential to develop multiple tumors, in particular meningiomas and BCCs.
1. Kiwilsza M, Sporniak-Tutak K. Gorlin-Goltz syndrome - a medical condition requiring a multidisciplinary approach. Med Sci Monit, 2012;18(9):RA145-53.
2. Manfredi M, Vescovi P, Bonanini M, Porter S. Nevoid basal cell carcinoma syndrome: a review of the literature. Int J Oral Maxillofac Surg. 2004;33(2):117-24.
3. Wicking C, Bale AE. Molecular basis of the nevoid basal cell carcinoma syndrome. Curr Opin Pediatr. 1997;9(6):630-5.
4. Farndon PA, Del Mastro RG, Evans DG, Kilpatrick MW. Location of gene for Gorlin syndrome. Lancet. 1992;339(8793):581-2
5. Baliga SD, Rao SS. Nevoid-basal cell carcinoma syndrome: a case report an overview on diagnosis and management. J Maxillofac Oral Surg. 2009;9(1):82-6.
6. Kimonis VE, Goldstein AM, Pastakia B, Yang ML, Kase R, DiGiovanna JJ, et al. Clinical manifestations in 105 persons with nevoid basal cell carcinoma syndrome. Am J Med Genet. 1997;69(3):299-308.
7. Morice-Picard F, Sévenet N, Bonnet F, Jouary T, Lacombe D, Taieb A. Cutaneous Epidermal Cysts as a Presentation of Gorlin Syndrome. Arch Dermatol. 2009;145(11):1341-3.
8. Shanley S, Ratcliffe J, Hockey A, Haan E, Oley C, Ravine D, et al. Nevoid basal cell carcinoma syndrome: Review of 118 affected individuals. Am J Med Genet. 1994.50(3):282-90.
9. Bale AE. The nevoid basal cell carcinoma syndrome: genetics and mechanism of carcinogenesis. Cancer Invest. 1997;15(2):180-6.
10. Cirrone F, Harris CS. Vismodegib and the hedgehog pathwqy: a new treatment for basal cell carcinoma. Clin Ther. 2012;34(10):2039-50.
The present study was carried out at the Instituto National do Cancer (INCA) - Rio de Janeiro (RJ), Brazil.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}