


Tatiana Gandolfi de Oliveira1; Rossana Cantanhede Farias de Vasconcelos2; Lilian Mayumi Odo3; Marina E.Y. Odo4
Keywords: KELOID; CICATRIX, HYPERTROPHIC; THERAPEUTICS; SKIN.
The first description of a treatment for keloids includes a mention of techniques dating back to 1,700 BC in Egypt. In 1806, Alibert used the term keloid to describe the lateral growth of tissue in injured skin. Such lesions result from the proliferation of dermal tissue after an injury of the skin 1 that extends beyond the borders of the original lesion - unlike hypertrophic scars, which are restricted to the limits of the trauma. 2 Keloids have a tendency to recur and generally do not spontaneously regress. 2-4
The proliferated tissue is the result of an increase of collagen and glycosaminoglycans.1 Its pathophysiology is poorly understood, and in addition to genetic and immunological factors.3-5 includes alterations in growth factors, collagen turnover, and tension in the affected area.
The tissue repair occurs in four stages. The first phase is the hemostasis. Immediately after the trauma, vasoconstriction occurs and the formation of the primary hemostatic plug takes place with platelets and the activation of the coagulation cascade. The second is the inflammatory phase, which lasts from the 1st to the 3rd day, when there is an increase of vascular permeability, stimulation of RNA, and the formation of collagen and endothelial changes occur. Erythrocytes, platelets, and polymorphonuclear leukocytes migrate to the lesion, promoting phagocytosis and degradation of collagen. The third is the proliferative phase, in which the production of collagen occurs. During this phase, which lasts from the 3rd to 24th day, any deficiency in the precursor elements of the healing process leads to changes in the formation of granulation tissue and to fibroblasts and neovascular proliferation. In the fourth phase, the remodeling phase, which can last from months to years, the collagen undergoes remodeling and forms a mature scar.6
The incidence of keloid formation affects around 4-16% of the population, includes all population groups, and while it is rare in newborns and the elderly, an increase in occurrence is seen in individuals between 10 and 20 years old, and in people of Asian and African descent.7
The management of keloids can be difficult and frustrating.5,7,8 Several therapeutic modalities have been indicated, including topical and intralesional corticosteroids, cryotherapy, surgery, laser procedures, silicone, radiotherapy, and other options on an experimental basis, such as: interferon, 5-fluorouracil, retinoids, verapamil, imiquimod, bleomycin, tamoxifen, tacrolimus, botulinum toxin and a promising therapy using transforming growth factor TGF-beta 3 and human recombinant interleukin-10, directed against the growth of collagen.
There is a trend towards individualization of treatment depending on the distribution, size, thickness, consistency of lesions, and presence of inflammation. 5,9 A combination of therapies seems to be the best option, 9 and, according to Leventhal et al. in a meta-analysis of multiple treatments, there was no statistically significant difference between them. 10
One of the main rules for the treatment of keloids is prevention, which can be carried out with the use of compression therapy, reducing the tension in scarring, thus avoiding unnecessary procedures in patients predisposed to scarring aberrations.1,3
Excisional surgery used as an isolated therapy has a recurrence rate of 45-100%, and is generally used in combination with other modalities, such as radiation therapy, interferon, corticosteroids, and imiquimod.1
There are few reports in the literature on the use of methotrexate as an alternative therapy for keloids. In a study by Muzaffar et al. in 2004,11 methotrexate was employed systemically in low doses for a short time after surgery for syndactyly. Also, a report by Onwukwe in 198012 discusses the systemic use of methotrexate associated with surgery.
The action of methotrexate takes place through competitive inhibition of the enzyme dihydrofolate reductase, which is responsible for the conversion of folic acid into tetrahydrofolate, with this cofactor being necessary for the transfer of carbon from many metabolic reactions, including the synthesis of purines bases and of thymidylate synthase. Cell proliferation is affected because it reduces the synthesis of thymidylate synthase and hence, of the nucleotide precursors that comprise DNA and RNA, affecting repair and replication of nucleic acids. Tissues with higher metabolic activity and increased cell growth are the most affected, which explains some pharmacological, secondary, and toxic effects. 11,12
To calculate the weekly dose, the authors used the fundamentals of treatment for psoriasis, in which the minimum dose of 2.5-5.0mg is used for maintenance. 13
To treat keloids with excision and intralesional injection of methotrexate.
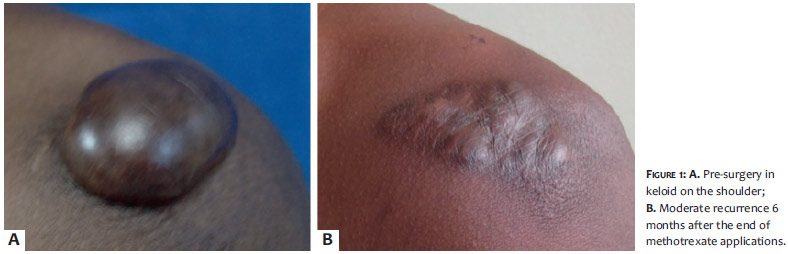
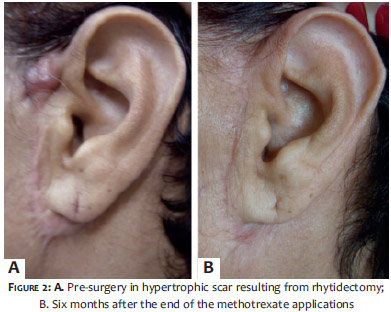
An open study of therapeutic intervention was carried out with 15 selected patients with keloids or hypertrophic scars (5 men and 10 women), who were treated at the ambulatory of the dermatology department of the Universidade Santo Amaro (Unisa), in São Paulo, Brazil. Four men and 6 women had keloids, and 1 man and 4 women bore hypertrophic scars. Eleven patients completed the study (9 women and 2 men). The body sites treated were: shoulder (Figure 1), periauricular (Figure 2), cervical, pre-sternal, abdominal, infraumbilical, supra-pubic abdominal (Figure 3), lateral dorsal, and lumbar regions, and the popliteal fossa. The study was conducted according to standards established by the institution's Ethics Committee.
The following examinations were performed in advance: blood count, AST, ALT, total bilirubin and fractions, urea, creatinine, CEA, Papanicolau test (in women), PSA (in men) and chest radiography. The examinations were carried out before the treatment, and 3 and 6 months after.
The lesion was completely excised in ellipse, with subcutaneous stitches combined with a continuous suture of the skin, having been removed after 4 weeks. The suture line was injected intralesionally with methotrexate from the 7th day after surgery, weekly for 6 months. The weekly dose was 2.5mg diluted in saline, in sutures of up to 10.0cm. No application with doses greater than 5.0mg/20cm was carried out. Prior to application, the skin was injected with 2% lidocaine to reduce the burning sensation caused by the drug.
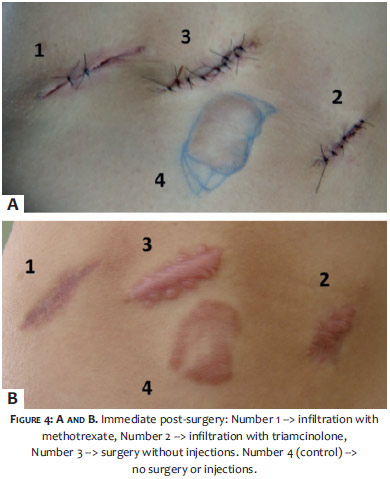
In one of the cases, the authors have chosen 4 keloid lesions of similar size in the same area to undergo surgical exeresis, with suturing of three lesions, leaving the fourth as a control (no surgery and injections). Of the 3 excised keloids, one received methotrexate, the other received intralesional corticosteroids (5.0mg triamcinolone), while the remaining was left without associated injections.
The analysis was performed with photographs being taken before, during, and after 6 and 12 months (Figure 4). Some cases returned up to 24 months after the completion of the treatment. The lesion was examined by the physician and the patient regarding the final aesthetic result.
Of the 15 selected cases, 4 patients withdrew from the study (1 woman and 3 men). Among the 11 treated cases there was a partial recurrence in 6, and no recurrence in 5 (2 keloids and 3 hypertrophic scars). None had a full recurrence. Partial recurrences were classified as minimal and moderate. The minimal recurrences took place in 2 cases (1 keloid and 1 hypertrophic scar), and the moderate recurrences totaled 4 (3 keloids and 1 hypertrophic scar -1 shoulder, 1 lateral dorsal, 2 pre-sternal).
Regarding the final aesthetical results, all cases showed an enlarged suture, even when leaving the external stitches for 4 weeks. An unsightly hyperpigmentation in the infiltrated area was observed in all cases, showing little whitening over six months of control.
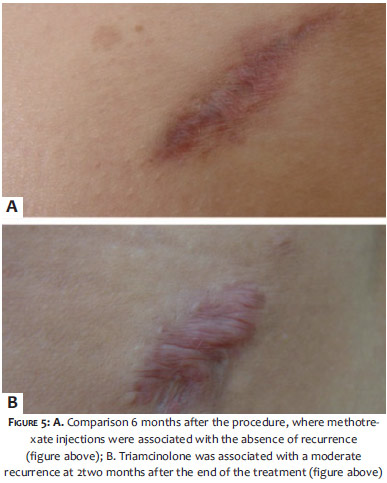
Regarding the case that had 4 lesions treated with 3 different methods and 1 control (a - surgery plus methotrexate injection, b - surgery plus corticosteroids injection, c -isolated surgery, and d - no surgery or injections), the results were: a - stable progress without recurrence, but with widening and hyper-pigmentation of the scar six months after the last methotrexate session; b - hypochromia and scar recurrence six months after the last session (Figure 5); c - keloid recurrence soon after surgery and coursing without recurrence up to six months after the procedure; d - unchanged progression.
None of the patients had alterations in the laboratory tests.
The present study is aimed at improving the aesthetics of hypertrophic scars and keloids. Occlusive silicones, injections of corticosteroids, cryosurgery, surgical excisions associated with beta therapy; and applications of CO2, Nd:YAG and dye lasers are the most common treatments in the daily practice to prevent aberrant scars, more or less effectively. 1
The present study used methotrexate injections for 6 months after the surgical excision of the lesions with a six-month follow-up after the end of the injections.
A recent study by Smith14 reports that there is still little information available about the natural history and prognosis of keloids formation. In its sample, the average number of years to achieve resolution of the keloids with treatment was. 11,4
The long period of applications in the present study hampered patient compliance, especially among men. The removal of stitches four weeks after surgery was due to the risk of dehiscence, even though there was widening of the scar. The dose used is 2.5mg (injectable vials of methotrexate have 50mg/2ml), i.e. 0.1ml is diluted in 0.9ml saline.
This dose is enough for scars without tension and up to 10.0cm in length. Due to the fact that the injection is very painful, previous injection with 2% lidocaine with epinephrine is recommended along the surgical scar. In larger lesions or in areas of tension, a maximum dose of 5.0mg per week is used, with no laboratory abnormalities being observed during and after the application of methotrexate, demonstrating safety for that dose. The authors also noted that the location of the keloid is important. In the pre-sternal region and in areas of tensioning, such as in the shoulder and in lateral dorsal region, there was moderate recurrence. Therefore, the dose of 2.5mg/10cm scar may be insufficient. There was 1 case in the sternal region where a partial recurrence occurred before the end of the sessions. Due to the small number of cases, it is not possible to state whether there is any difference in outcomes between genders and between the two types of lesions approached. Leventhal 10 led a meta-analysis looking for the best treatment for keloids and hypertrophic scars, in a review of 70 studies from the literature available up to October 2005, concluding that 60% of cases result in improvement with treatment and that there is no statistically significant difference between them. It also concluded that most treatments result in little probability of improvement and even patients who go through long periods of controlled clinical symptoms would be far from cured.
In the case where the progression of keloids treated with steroids was compared with controls, the authors noted that methotrexate presented better stability of the scar as compared with those treated with corticosteroids after the end of the applications. The scar injected with corticosteroids developed with mild atrophy and hypochromia until the last session, however the recurrence began 2 months after the end of the treatment, completing at 6 months. This case was followed up with for 2 years after the completion of the treatment, with the results remaining unchanged. Other resources can be employed using comparative treatments with a greater number of cases.
The application of 2.5mg methotrexate for every 10cm of scar after surgical excision of keloids or hypertrophic scars in 11 treated cases, resulted in an absence of recurrence in 5 cases; partial recurrence in 6 (minimal in 2 and moderate in 4 cases). No full recurrence was observed. The cases were followed up with for 6 months after the end of the applications. The maximum dose of 5.0mg was proved to be safe up until 6 months after the end of the treatment, with no alterations in laboratory tests. Further studies are necessary to complement this analysis.
1. Berman B, Flores F. The treatment of hypertrophic scars and keloids. Eur J Dermatol.1998;8(8):591-5.
2. Gailloud-Matthieu MC, Raffoul W, Egloff DV. Hypertrophic scars and keloids: which therapeutic options today?. Rev Med Suisse Romande. 1999;119(9):721-8.
3. Uriost SS, Arndt KA, Dover JS. Keloids and hypertrophic scars: review and treatment strategies. Semin Cutan Med Surg. 1999;18(2):159-71.
4. Lee Y, Minn KW, Baek RM, Hong JJ. A new surgical treatment of keloid: keloid core excision. Ann Plast Surg. 2001;46(2):135-40.
5. Al-Attar A, Mess S, Thomassen JM, Kauffman CL, Davison SP. Keloid pathogenesis and treatment. Plast Reconstr Surg. 2006;117(1):286-300.
6. Gonçalves G, Parizotto NA. Fisiopatologia da reparação cutânea: atuação da fisioterapia. Rev Bras Fisiot. 1998;3(1):5-13..
7. Brudnik U, Podolec-Rubi M, Wojas-Pelc A. Therapeutic problems connected with keloid treatment-new treatment possibilities. Przegl Lek. 2006;63(9):803-6.
8. Hackert L, Aschoff R, Sebastian G. The treatment of keloids. Hautarzt. 2003;54(10):1003-15.
9. Mutalik S. Treatment of keloid and hypertrophic scars. Indian J Dermatol Venereol Leprol. 2005;71(1):3-8.
10. Leventhal D, Furr M, Reiter D. Treatment of keloids and hipertrophic scars: a meta-analysis and review of literature. Arch Facial Plast Surg. 2006;8(6):362-8.
11. Muzaffar AR, Rafols F, Masson J, Ezaki M, Carter PR. Keloid formation after syndactyly reconstruction: associated conditions, prevalence, and preliminary report of a treatment method. J Hand Surg Am. 2004;29(2):201-8.
12. Onwukwe F. Treating Keloids by Surgery and Methotrexate. Arch Dermatol. 1980;116(2):158.
13. Marques AS. Metotrexate na psoríase. Consenso Brasileiro de Psoríase. Rio de Janeiro: Sociedade Brasileira de Dermatologia; 2009. p. 63-8.
14. Smith OJ, McGrouther DA. The natural history and spontaneous resolution of keloid scars. J Plast Reconstr Aesthet Surg. 2014;67(1):87-92.
The present study was carried out at the Department of Dermatology of the Universidade de Medicina de Santo Amaro (UNISA) - São Paulo (SP), Brazil.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}