


Maria Cristina Cardoso de Mendonça1; Maria Gabriela Araújo Lopes2; Rosana Rocon Siqueira2; Fernanda Queiroz de Oliveira3; Gianne Pascoal3; Aloísio Carlos Couri Gamonal4
Keywords: FACIAL ASYMMETRY; FACIAL PARALYSIS; QUALITY OF LIFE; BOTULINUM TOXINS, TYPE A.
Craniofacial paralyses and dyskinesias trigger functional and aesthetic changes, which cause physical and psychological disorders. In the case of facial paralysis, there is excessive contraction of the contralateral side to the paralyzed side, due to the fact that there is no effective opponent musculature. The non-paralyzed side shows deviation of nasal, labial, and orbital regions, even when the muscles are at rest. Thus, rotation of the face towards the side not affected by paralysis takes place, causing shortening of that hemiface. The treatment of the resulting facial asymmetry aims at restoring muscle balance and regaining symmetry when in states of rest and motion. 1,2
Surgical techniques are ineffective most of the time, and in addition present risk of complications.2 Due to its safety, effectiveness and good tolerance levels, botulinum toxin type A therapy becomes a good option in the treatment of these pathological conditions, with the advantage of being made available by the Brazilian National Health System (SUS).3,4 It has been used to treat synkinesis,5 hyperlacrimation,6 hyperkinesias,7 and sequelae in the frontal and mandibular regions secondary to rhytidectomy.8 The results have been so significant, that is has been considered by many to be the best treatment for the motor and autonomic effects caused by aberrant neural regeneration.6 Based on the skill of the dermatologist - gained with the application of botulinum toxin in their daily practice for the treatment of various skin disorders such as facial aging - with this study the authors aim at demonstrating the safety and efficacy of this procedure when performed by an experienced professional, as well as the clinical improvement and degree of satisfaction of the patients who undergo it.
A non-randomized parallel study, was carried out at the Dermatology Service of the Hospital Universitário da Universidade Federal de Juiz de Fora (UFJF), in the southern Brazilian State of Minas Gerais. It included 12 patients with facial asymmetries who were referred by the Dermatology Ambulatory or by other specialties, from January 2011 to December 2013.
Patients with significant facial asymmetries or dyskinesias, who had not undergone previous treatment, between the ages of 20 and 80 years, and not bearers of neuromuscular diseases, were selected.
The product used in the study (Botox®, Allergan Pharmaceuticals, Irvine, California, U.S. and Prosigne®, Lanzhou, Institute Biological Products, China) was supplied by the SUS. According to the needs of each patient, the toxin was applied in individualized doses in order to weaken the facial muscles in the hemiface not affected by the paralysis, and directly into the muscle responsible for the dyskinesia. Clinical assessments were carried out on the first day of the procedure (D0) and 15 days after (D15). The patients were photographed at each visit in static and dynamic standardized positions, using the same digital camera and ambient lighting (Figures 1 to 3). Each patient was rescheduled for a future visit within 120 days of the last application. The study followed the ethical guidelines issued by the Helsinki Declaration of 2000, revised in 2008.
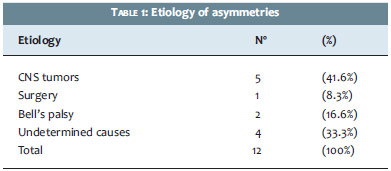
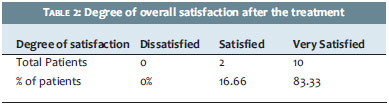
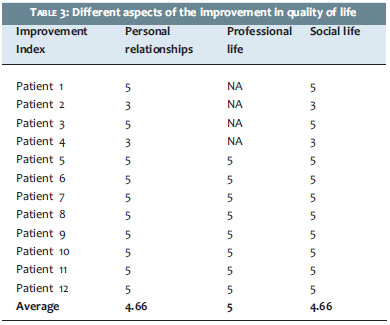
The 12 selected patients had a mean age of 56.4 years. Nine (75%) were females and 3 (25%) males. The etiology of asymmetries included tumors of the central nervous system, surgeries, Bell's palsy and indeterminate causes (Table 1). The total number of doses in each application varied according to individual needs (between 8.2 and 51 units per application). Patients were questioned about their overall degree of satisfaction after the treatment (Table 2) and were asked to rate their level of satisfaction with different aspects of their daily lives, using a scale varying from 1 to 5 (1 = mild improvement and 5 = great improvement). In the evaluation regarding the impact on professional life, the expression "not applicable (NA)"was used for patients already retired from their work activities (Table 3). A high level of patient satisfaction, as well as improvements in their personal relationships and social and professional lives, were observed after the correction of the asymmetries. Regarding complications, 2 cases of lagophthalmos and 1 of headache were verified. These symptoms were transient and did not cause inconvenience to patients.
Facial palsy and craniofacial dyskinesias trigger changes in speech, smile, swallowing, and chewing, and can cause serious damage to the patient's ability to express emotions and their own image.1,3 In facial paralysis, the unaffected muscles become hyperkinetic, generating an imbalance based on the inaction of the opponents muscles.1,2 Dyskinesias are defined as involuntary movements of the muscles of the face and neck, including blepharospasm, characterized by involuntary spasmodic bilateral closing of the eyelids9 and hemifacial spasm, which consists of tonic-clonic unilateral contraction and of muscles innervated by the facial ipsilateral nerve. They are often accompanied by other sensory (visual or auditory disorders), motor (weakness of the facial muscles, trismus, bruxism, dysarthria) and/or autonomic (lacrimation and salivation) alterations. Muscle spasms start in the periocular region and progress to the perioral region and masticatory muscles. 10
The main etiologies of facial asymmetry include strokes, surgical lesions, traumatic lesions, Bell's palsy, intracerebral tumors, and paralysis of undetermined etiology. 2 The treatment of facial paralysis aims at restoring the symmetry, in the static and dynamic state, that is seriously affected by progressive contralateral hyperkinesis. 1,2 A good treatment option is botulinum toxin type A due to the fact that it is safe, effective, and well tolerated. It is considered the treatment of choice for hemifacial spasm. 11 In the literature there are few reports by dermatologists on the treatment of facial asymmetry with the use of botulinum toxin, despite the fact it has been used since the 1970s to treat a number of conditions related to abnormal muscular contractions. 3,4 It works by blocking the release of acetylcholine at the neuromuscular junction, which prevents contraction of the muscle. 3,12 In hemifacial spasm, it is used directly in the affected muscle, blocking its involuntary action. It has been used for the treatment of facial hyperkinesia on the side not affected by paralysis, with the need for a higher total dose being described, however with a similar duration of action when used for other purposes.3 In the present study, the number of units ranged between 8 and 51, with periodic reapplication after an interval of 90 to 120 days after the previous session.
Adverse events are rare with injections of the toxin to the face and are associated with the use of high doses.12 In the present study there were no early complications, such as hematoma, infection, or allergy to the toxin, nor irreversible complications. Of all the patients who were evaluated, the authors evidenced transient complications in 3 of them, with 2 presenting lagophthalmos and 1 headache. There was improvement in the mobility of the side affected by paralysis, as a secondary effect to the application of botulinum toxin in the uninvolved side. The various etiologies of facial asymmetries, the variety in the anatomy, and the strength of the musculature make it difficult to standardize the injection points and the amount of units to use in each of them, indicating that the experience of the professional carrying out the application is an important factor.13 The use of botulinum toxin in the field of cosmiatry allowed the dermatologist to originally master its use. In line with the results obtained in the present study, the combination of this knowledge with the great aesthetic insight gained by dermatologists throughout his or her clinical practice reinforces the idea that such a professional is able to successfully treat such patients. The treatment of asymmetries is extremely rewarding, as it provides patients with reintegration and selfacceptance. The degree of patient satisfaction is high in contrast to the low rate of adverse effects. 1-3
Botulinum toxin type A has proved to be an important alternative in the treatment of facial asymmetries. It contributes to improved self-image and self-expression, and leads to a positive social impact and improved quality of life for patients undergoing the treatment. Dermatologists are able to successfully treat such imperfections as evidenced by the clinical improvement, high degree of satisfaction of patients undergoing the procedure, and the few and limited adverse events. Nevertheless, more comprehensive studies, carried out by dermatologists, are necessary to consolidate the ability of such professionals to treat facial asymmetry with botulinum toxin.
1. Maio M. Therapeutic uses of botulinum toxin: from facial palsy to autonomic disorders. Expert Opin Biol Ther. 2008;8(6):791-8.
2. Domingos MM. O uso da Toxina botulínica em pacientes com hipercinesia muscular facial contralateral à paralisia facial (tese). São Paulo: Universidade de São Paulo; 2006.156 p.
3. Sadiq SA, Khwaja S, Saee SR. Botulinum toxin to improve lower facial symmetry in facial nerve pals. Eye (Lond). 2012;26(11):1431- 6.
4. Jandhyala R. Impact of Botulinum Toxin A on the Quality of Life of Subjects Following Treatment of Facial Lines. J Clin Aesthetic. 2013;6(9):41-5.
5. Badarny, S., Giladi, N., Honigman, S. Botulinum toxin injection effective for post peripheral facial nerve palsy sinkenesis. Harefuah. 1998;135(3-4):106.
6. Boroojerdi B, Ferbert A, Schwarz M, Herath H, Noth J. Botulinum toxin treatment of synkinesia and hyperlacrimation after facial palsy. J. Neurol. Neurosurg. Psychiatr.1998;65(1):111-4.
7. Dressler D,, Schonle PW. Hyperkinesias after hypoglosso facial nerve anastomosis-treatment with Botulinum toxin. Eur. Neurol. 31(1):44,1991.
8. Clark RP, Berris CE. Botulinum toxin: a treatment for facial asymmetry caused by facial nerve paralysis. Plast Reconstr Surg. 1989;84(2):353-5.
9. Carvalho RMSL, Gomi CF, Carvalho ALS, Matayoshi S, Moura EM. Tratamento do blefaroespasmo e distonias faciais correlatas com toxina botulínica - estudo de 16 casos. Arq Bras Oftalm. 2003;66(1):13-6.
10. Auger RG, Whisnant JP. Hemifacial spasm in Rochester and Olmsted County, Minnesota, 1960-1984. Arch Neurol. 1990;47(11):1233-4.
11. Frei K, Truong DD, Dressler D. Botulinum toxin therapy of hemifacial spasm; comparing different therapeutic preparations. Eur J Neural. 2006;13(Suppl 1):30-5.
12. Armstrong MW, Mountain RE, Murray JA. Treatment of facial asymmetry with Botulinum toxin type A following facial nerve palsy. Clin. Otolaryngol. 1996;21(1):15-20.
13. Salles AG, Toledo PN, Ferreira MC. Botulinum toxin injection in long- standing facial paralysis pacients: improvement of facial symmetry observed up to 6 months. Aesth Plast Surg. 2009;33(4):582-90.
The present study was carried out at the Núcleo de Pesquisa em Dermatologia (Nupede) do Hospital Universitário da Universidade Federal de Juiz de Fora (UFJF) – Juiz de Fora (MG), Brazil.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}