


Osório Alves Corrêa de Castro Lara1; Ed Wilson Tsuneo Rossoe2
Keywords: HYPERHIDROSIS; AXILLA; DERMATOLOGIC SURGICAL PROCEDURES; SWEAT GLANDS.
Primary axillary hyperhidrosis is characterized by excessive sweating in physiologically larger quantities than that needed for thermoregulation, being considered most often of idiopathic etiology. It has a major impact on quality of life, with limitations on professional life, social interaction, physical activity, and leisure. Its prevalence varies from 1-3% in the population, with a slight predominance in people of Jewish and Asian origin.1-4
The treatment of axillary hyperhidrosis may be carried out conservatively with topical products, medicaments, iontophoresis, and botulinum toxin. When the clinical options do not present satisfactory results, surgical procedures are indicated, with a preference for localized resection. Comparatively, transthoracic sympathectomy has a higher risk of complications, such as chest wall paresthesia (50%), pneumothorax (7%), Horner's syndrome (<1%), and hemothorax (<1%), in addition to compensatory sweating in other body sites.3-6
Local resection of the skin and subcutaneous tissue was used for many years, since the complete exeresis of the sweat glands guaranteed the definitive solution to hyperhidrosis, however it frequently entailed scars with fibrosis and restriction of movement. On the other hand, the removal of the glandular tissue without resection of the skin can be performed through curettage or ablation in a "blind" way (without visual control) - as it is done in liposuction with curettage - or under visual control, usually with the eversion of the borders of the surgical wound in order to visualize the glandular tissue. These two techniques provide additional options for axillary hyperhidrosis resistant to clinical treatment, besides having less morbidity when compared with the already mentioned surgical techniques.3, 6-9
A 26-year-old mulatto female patient with a history of excessive axillary sweating for five years sought care at the dermatology service. She described noticing the onset of the condition after taking a daytime job as a keeper of an uncovered parking lot, where she had to wear a black-colored uniform. Due to the need for frequent changes of the uniform during the work shift because of excessive sweating, she decided to seek care. Once diagnosed with axillary hyperhidrosis, a treatment with aluminum hydrochloride associated with botulinum toxin was administered with excellent results during the first six months. Nevertheless, after one year of treatment the patient's condition worsened. She was then referred for local surgery, with procedures performed in each of the axillae during different months.
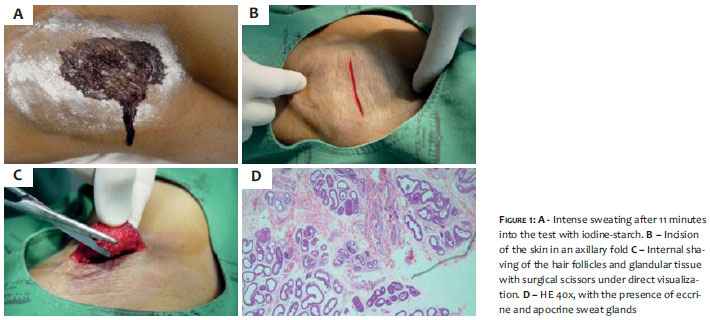
The patient, who had suspended the use of topical products in the axillae for five days, was placed in the operating room in the supine position, at a room temperature of 21ºC. The demarcation of the hyperhidrotic area was carried out through the Minor iodine-starch test (Figure 1a), with subsequent local antisepsis with pyrrolidone iodine solution and local anesthesia of the affected area. An incision was performed in the axillary crease aligned with the tissue's tension lines (Figure 1b). The detachment of the skin was carried out in the subcutaneous plane, being followed by rigorous hemostasis with electrocoagulation. The borders of the wound were everted, and under direct visual observation, the shaving of the dermis was conducted with surgical scissors, (Figure 1c) with the material removed being sent for histological study (Figure 1d). After the procedure, the skin was sutured with 4-0 nylon, with the placement of a penrose drain. A dressing was applied until the following day.
On the first post-operative day, the penrose drain was removed, with no local complications - such as bleeding, hematoma, necrosis, infection, seroma, or dehiscence - being observed. The patient was instructed as to local care of the surgical wound, antibiotic therapy with cephalexin for 7 days, and restriction of vigorous exercise with the upper limbs for the same period.
The reassessment of the sweating was performed using the iodine-starch test after the procedure, at 14 months in the right axilla and at 16 months in the left axilla, with no sweating being observed in the right axilla (Figure 2a) and a discrete area of residual sweating in the left axilla (Figure 2b).
In axillary hyperhidrosis, 50% of the sweat is produced by apocrine glands and 50% by eccrine glands. Using the shaving technique with surgical scissors, the target is the deep dermis and the subdermis, which is the most superficial part of the subcutaneous. In this way, two types of glands are removed: the apocrine (that are located closely adjacent to the hair follicles) and the eccrine (that are partially removed, except for the complete removal of the dermis).7
Ideally, the permanent removal of axillary sweat glands results in permanent improvement of hyperhidrosis. However, the limited data regarding the results of curettages and the variations in surgical techniques do not allow definitive conclusions on the effectiveness of the procedure in the long run. Continued sweating may occur as a result of incomplete removal of eccrine glands in certain areas or due to local compensatory sweating. The skills of the surgeon performing the procedure can also influence the treatment's efficacy.
The final cosmetic result was considered good, showing no cicatricial retraction. The local sensitivity was preserved, and there was a decrease of the axillary hairs, which was not cause for dissatisfaction by the patient.
The authors consider the described surgical technique for axillary hyperhidrosis as a safe method, with low complication rates and an excellent additional option for cases where there is resistance to conservative treatments. Due to the fact that the study was carried out with only one case, the authors note that recurrences cannot be excluded for the method.l
Acknowledgements:
The authors would like to thank Dr. José Antonio Tebcherani (for the photograph of the histopathological examination) and Dr. Luiz Horta Cristiano de Lima Junior (for the examination's report).
1. Hornberger J, Grimes K, Naumann M, Glaser DA, Lowe NJ, Naver H, et al. Recognition, diagnosis, and treatment of primary focal hyperhidrosis. J Am Acad Dermatol. 2004;51(2):274.
2. Fenili R, Fistarol ED, Delorenze LM, Demarchi AR, Matiello M. Prevalência de hiperidrose em uma amostra populacional de Blumenau-SC, Brasil. An Bras Dermatol. 2009;84(4):361-6.
3. Gontijo GT, Gualberto GV, Madureira NAB. Atualização no tratamento de hiperidrose axilar. An Bras Dermatol. 2011;3(2):147-51.
4. He J, Wang T, Dong J. Excision of apocrine glands and axillary superficial fascia as a single entity for the treatment of axillary bromhidrosis. J Eur Acad Dermatol Venereol. 2012;26(6):704-9.
5. Haider A, Nowell S. Focal hyperhidrosis: diagnosis and management. CMAJ. 2005;172(1):69-75
6. Coelho MC, Lira EJT, Zanin AS, Gonçalves JL, Neto NB, Júnior WSS. Simpatectomia torácica por videotoracoscopia no tratamento da hiperidrose palmar e axilar. An Bras Dermatol. 2002;77(2):171-83.
7. Odo MEY, Chichierchio A. Curetagem cirúrgica das glândulas sudoríparas (endoshave axilar). In: Hexsel DA, Almeida ART. Hiperidrose e toxina botulínica. 2003. p.121-24.
8. Bechara FG, Sand M, Hoffmann K, Altmeyer P. Aggressive shaving after combined liposuction and curettage for axillary hyperhidrosis leads to more complications whithout further benefit. Dermatol Surg. 2008;34(7):952-3.
9. Stori WS, Neto NB, Coelho MS, Pizarro LDV, Guimarães PSF. Bloqueio por clipagem de gânglios simpáticos torácicos no tratamento da hiperidrose. An Bras Dermatol. 2006; 81(5): 425-32.
The present study was carried out at Complexo Hospitalar Padre Bento de Guarulhos - Guarulhos (SP), Brazil.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}