


Marcela Duarte Villela Benez1; Deborah Sforza2; Danielle Mann3; Solange Cardoso Maciel Silva4
Keywords: CARCINOMA, BASAL CELL; CARCINOMA, SQUAMOUS CELL; MOUTH MUCOSA; EYELID NEOPLASMS; SURGICAL FLAPS.
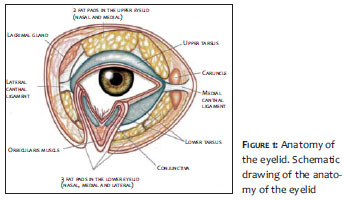
The moveable nature of the eyelids and their functional and aesthetic importance create substantial challenges for the reconstruction of this structure after surgery for tumor resection. A detailed understanding of the anatomy of the eyelid and ocular areas (Figure 1) helps the surgeon in selecting the best surgical technique for restoring ocular function and improving the aesthetic result.
The eyelid is divided into anterior and posterior lamella. The anterior lamella consists of skin and the orbicularis muscle. The posterior lamella consists of the conjunctiva, tarsus, and the eyelid retractor muscles. The orbital septum can be considered a middle lamella and cannot usually be rebuilt.1-3 The ocular conjunctiva on the surface of the eyeball is continuous with the conjunctiva that overlays the inner surface of the eyelids. This relationship needs to be maintained or restored during reconstruction in order to preserve the palpebral function and prevent complications, such as dryness of the cornea, keratitis, and finally, loss of vision.
The selection of the best technique will depend on the size of the surgical wound, its location, and depth.2
Superficial surgical defects require only reconstruction of the anterior lamella. Full-thickness defects require that both lamellae - anterior and posterior - be reconstructed.2
Direct primary closure of the eyelid is sometimes possible in the presence of deformities of up to 33% of its horizontal length.
A wedge excision of the total thickness is carried out, and subsequently comes close to the vertical edges of the vertical matress suture. However in major defects, it gives preference to flaps instead of grafts. In this case1-5, different types of skin flaps can be used: advancing; transposition; Mustardé and Mcgregor; Fricke,6 Landolt-Hughes, Dupuys-Dutemps Hughes (uses skin and mucosa of the upper eyelid); and Abbe.1, 3, 7
The present article is aimed at introducing a technique for the reconstruction of the posterior lamella, only with a jugal mucosa graft and a Mustardé or a cutaneous advancement flap.
A group of 6 patients - between 52 and 73 years of age, bearing surgical wounds on the lower eyelid, resulting from the removal of malignant tumors that were larger than two thirds (50%) of the eyelid's horizontal extension. The tumors were previously confirmed by histopathology: 5 basal cell carcinomas (BCC) and 1 squamous cell carcinoma (SCC). (Table 1) The patients were photographed by the same professional photographer at the pre- and post-operative stages, with the same technique and camera.
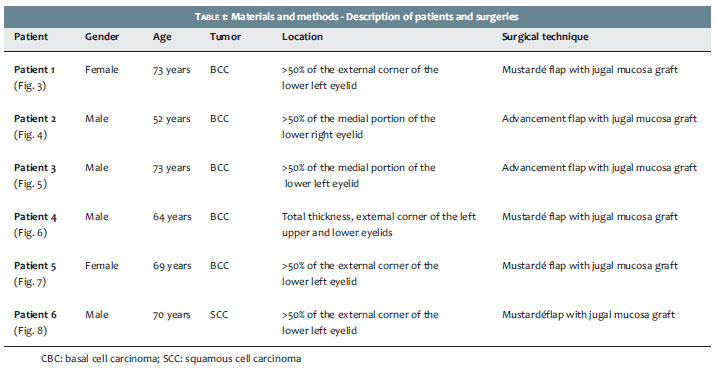
The patients underwent local anesthesia with a tumescent solution. After the complete excision of the tumor located in the lower eyelid, surgical reconstruction was performed with a cutaneous advancement or Mustardé flap. For the reconstruction of the posterior lamella, the authors used only the jugal mucosa. In all 6 cases the reconstruction of the tarsus with cartilage graft - which is usual in the lower eyelid surgeries with extensive involvement of that anatomical structure - was not carried out. (Figure 2)
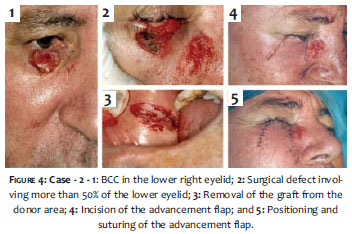
The reconstruction using the advancement flap consists of carrying out a composite flap with 2 vertical and parallel incisions, with a number 15 scalpel blade, just below the surgical defect. The subcutaneous tissue is detached at the orbicularis muscle level. The jugal mucosa graft is removed and then positioned in the residual conjunctiva, being sutured with absorbable thread (6.0 catgut). Next, the cutaneous flap is completely detached, superiorly advanced, and positioned within the deformity of the lower eyelid in such a way that the upper border of the residual tarsus is aligned with the border of the flap. The skin is then approximated with a simple suture of 6.0 mononylon thread.
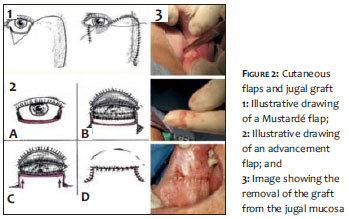
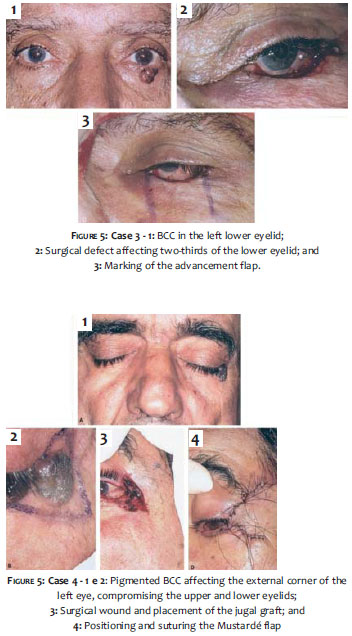
For reconstruction using the Mustardé technique, a lateral incision is carried out from the external canthus - at the level of the zygomatic arch - and running upwards in the direction of the temporal region. The skin is completely detached up to the orbicularis muscle. The jugal mucosa graft is subsequently attached to the residual conjunctiva with absorbable suture (6.0 catgut). Then the musculocutaneous flap is positioned on the lower eyelid, the edges of the wound are brought closer to each other, and the external canthal ligament is sutured to the periosteum for the fixation of the lower eyelid. The skin is then sutured with simple continuous stitches using 6.0 mononylon thread.
A 73-year-old female patient with BCC located in the external corner of the left lower eyelid, covering 50% of its length. The authors have chosen the Mustardé technique, with the use of a jugal mucosa graft. (Figures 2 and 3)
A 52-year-old male patient with ulcerated nodular BCC on the right lower eyelid, involving more than 50% of its medial portion. The grafting with jugal mucosa and advancement flap was chosen for the replacement of the anterior lamella, as the location of the tumor was medial. (Figure 4)
A 73-year-old male patient with ulcerated nodular BCC on the left lower eyelid, in its medial portion. The lesion affected approximately two-thirds of the eyelid. The authors have again chosen the advancement flap and grafting with jugal mucosa of the conjunctiva. (Figure 5)
A 64-year-old male patient with nodular BCC affecting the external canthus of the left eye in the total thickness of the upper and lower eyelids. A Mustardé flap and a jugal mucosa graft were performed with excellent functional and aesthetic outcomes. (Figure 6)
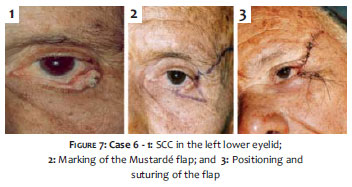
A 69-year-old female patient with nodular BCC in the external portion of the left lower eyelid, covering two-thirds of its length. In this case, a Mustardé flap and a jugal mucosa graft were also performed with good outcomes. (Figure 7)
A 70-year-old male patient with an SCC affecting two-thirds of the external region of the left lower eyelid. The authors have chosen reconstruction with a Mustardé flap and a jugal mucosa graft. (Figure 8)
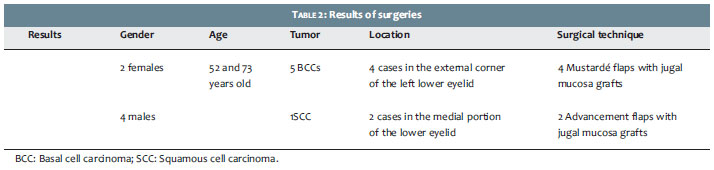
Six patients (aged 52-73 years, 2 females and 4 males, 5 diagnosed with BCC and 1 with SCC) were operated on. Among the operated cases, 4 were located at the external corner of the left lower eyelid (with 1 of these affecting both the external corners of the upper and the lower left eyelids. The 2 remaining cases affected the medial portion of the lower eyelid.
The patients who had the external corner of the lower eyelid compromised by the tumor underwent the Mustardé flap techniquewith graftsof oral mucosa. On the other hand, the patients with involvement of the medial portion of the lower eyelid underwent an advancement flap with oral mucosa graft. (Table 2)
The 6 patients had no major complications during the post-operative period. Palpebral oedema with difficulty opening the eye and slight hematoma are expected in the first days after surgery, usually resolving in a few days. All patients received prophylactic antibiotics and were instructed to carry out compress with ice and rest with the head elevated, in order to decrease the palpebral oedema. The stitches were removed on the 7th postoperative day.
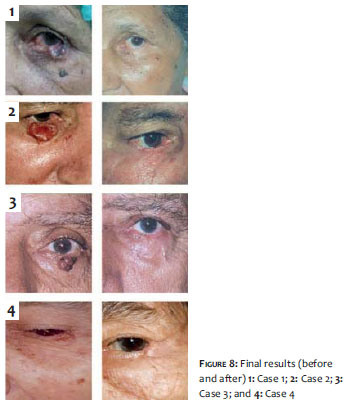
It has been more than 7 years since these patients were operated on and all continue to be monitored at the Dermatologic Surgery Service. To date all have presented good aesthetic and functional outcomes in the lower eyelids, with the preservation of the anatomy of that region and without complications, such as keratitis and ectropion (Figure 8), in addition to having demonstrated satisfaction with the aesthetic and functional results of the performed surgery.
Several techniques have been described for the surgical reconstruction of the lower eyelid. In extensive surgical defects it is considered that the substitution of the conjunctiva for other mucosal tissue is necessary in order to avoid trauma to the cornea. The literature recommends replacing the tarsus with cartilage - aiming at restoring the palpebral skeleton function - and rebuilding the orbicular skin-muscle complex with a flap or graft.2, 4
The Mustardé technique was described during the Second World War and even today is considered one of the best options for extensive lesions in the lower eyelid. Despite the advancement flap not usually being performed in these surgical reconstructions, due to the risk of ectropion, they can provide satisfactory results as shown in our set of cases.1
The graft for reconstructing the tarsus is usually extracted from the nasal or auricular cartilage, or from the periosteum, with more recent descriptions of the use of the posterior temporal fascia. In the cases described, a choice was made for using only jugal mucosa for the repair of the conjunctiva, without the replacement of the tarsus, since in the presence of the remaining tarsus - both medial and lateral - the lower eyelid would remain properly positioned, avoiding the formation of both ectropion and entropion. The jugal mucosa was preferred at the expense of the mucosa of the palate due to the greater ease and lower incidence of complications at the donor site, such as oronasal fistula.1, 4, 8
By following these patients, the authors conclude that the procedure is safe and without anatomical and functional complications, and can be reproducible.
1. Silva SCMC. Cirurgia dermatológica - Teoria e prática. Rio de Janeiro: Dilivros; 2008.
2. Baker SR. Retalhos locais em reconstrução facial. 2º ed. Rio de Janeiro: Dilivros; 2009.
3. Strauch B, Vasconez LO, Findlay EJH. Grabb's encyclopedia of flaps. New York: Lippincott-Raven; 1998.
4. Maniglia R, Maniglia JJ, Maniglia F, Soccol A, Dolci JE. Técnica de compartilhamento pálpebral com retalho tarsoconjuntival para lamela interna na reconstrução palpebral inferior. Experiência de 32 casos. Acta ORL/ Técnicas em Otorrinolaringologia. 2007;25(3)204-11.
5. Lima EVA. Enxertia de tecido palpebral na reconstrução de tumores cutâneos. Surg Cosmet Dermatol. 2010;2(4)333-5.
6. Neto GH, Sebastiá R, Viana GAP, Machado F. Reconstrução palpebral com retalho de Fricke: relato de dois casos. Arq Bras Oftalmol. 2006;69(1):123-6.
7. Galimberti G, Ferrario D, Casabona GR, Molinari L. Utilidade do retalho de avanço e rotação para fechamento de defeitos cutâneos na região malar. Surg Cosmet Dermatol2013;5(1):769.
8. Fernandes JBVD, Nunes TP, Matayoshi S, Moura EM. Enxerto de mucosa do palato duro: complicações na área doadora - Relato de Casos. Arq Bras Oftalmol. 2003;66(6):884-6.
The present study was carried out at Hospital Universitário Pedro Ernesto da Universidade Estadual do Rio de Janeiro (UERJ) - Rio de Janeiro (RJ), Brazil.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}