


Petra Pereira de Sousa1; Carlos Alberto Chirano Rodrigues2; Renato Cândido da Silva Júnior2; Carolina Chrusciak Talhari Cortez2; Danielle Cristine Westphal1
Keywords: CARCINOMA, BASAL CELL; SURGICAL FLAPS; RECONSTRUCTIVE SURGICAL PROCEDURES
The nasal pyramid is the most common site for the emergence of malignant tumors in the head and neck, particularly in areas with great exposure to the sun, such as the nasal alae (45%), the nasal dorsum (17%) and the nasal tip (5.5%). 1 Basal cell carcinoma (BCC) is the most common malignant neoplasia, accounting for approximately 75% of those lesions, followed by squamous cell carcinoma (SCC), which accounts for 15% of cases and, more rarely, by melanoma, which in dermatology corresponds to 4% of all cutaneous malignancies.2
The reconstruction of surgical defects caused by the excision of nasal tumors is a challenge for dermatologic surgeons, due to the complex anatomy and limited availability of remaining skin in the site to perform the correction.2,3
Burget & Menick revolutionized nasal reconstruction surgery with the introduction of the concept of aesthetic subunits of the nose, based on differences in the skin's elasticity, color, contour and texture, contributing to the refinement of nasal surgery.4
Total thickness skin grafts can yield good results, however there is risk of depressed scars, dyschromias, and alterations in the shape of the nose. The results obtained with pedicled flaps are always superior than those obtained with grafts, precisely due to the reduction of those risks. 5 In the present study the authors present a method for the reconstruction of the alae, tip, and columella of the nose using a pedicled interpolated frontal flap after the excision of a BCC involving those subunits.
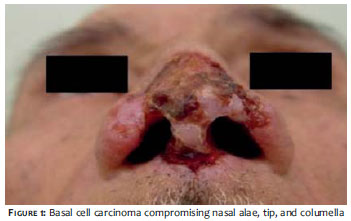
A 70-year-old Caucasian patient, originally from a rural area of the Northern Brazilian State of Amazonas, sought medical care complaining of a slow growing sore in the nasal tip, which had emerged one year before. The clinical examination evidenced an exulcerated and crusted plaque with pearly borders, of terebrant aspect, located in the nasal tip and alae, with invasion of the upper third of the columella. (Figure 1)
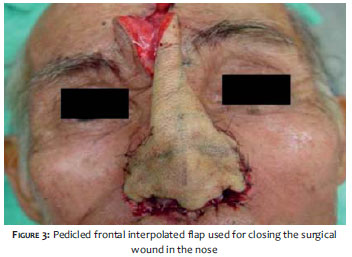
Histopathological examination confirmed the clinical hypothesis of BCC. Surgical excision with a 5 mm margin resulted in the bilateral removal of the nasal alae and columella. (Figure 2) The preparation of the flap used the paramedian frontal region as donor area. The flap was dissected in the subcutaneous plane up to the medial-lateral glabellar region. Doppler examination was not used to identify the supratrochlear artery. The closure process of the donor area was then performed by approximation. The portions in this area that could not be completely approximated were left to heal by second intention. No cartilage structure was used for remodeling the nose. (Figure 3) The second surgical event - which comprised the transection of the pedicle - was carried out four weeks after. Calcium alginate was used in the dressing. The surgical margins were free of the tumor and the patient recovered uneventfully and with excellent cosmetic result. (Figure 4)
The cutaneous flaps used for nasal reconstruction have great versatility in their application.1 Numerous techniques can be used for the closure of surgical defects caused by the excision of tumors in the nose, such as the primary synthesis, advancement flap, transposition flap, bilobed flap, grafts, or combinations of techniques. 3
The frontal region skin is recognized as the best donor area for nasal coverage, due to the appropriateness of its color and texture, with the interpolated frontal skin flaps used to treat great losses of substance affecting more than one aesthetic unit, and defects that affect cartilage and/or the mucosa.1,6 Furthermore, the arterial blood flow concept and venous drainage are of utmost importance for the design of the flap. The forehead is nourished by a rich vascular network supplied by the supratrochlear, supraorbital, and superficial temporal arteries.7 In the case described, the patient had full thickness compromise with involvement of the nasal alae, columella, and tip due to BCC.
The post-operative difficulties are most present in the first 24 hours, when the patient needs to remain with the nostrils occluded due to the dressing, and in the need for a second surgical event for the resection of the pedicle - which must be carried out four weeks later. As disadvantages of the technique, the authors highlight the presence of frontal scarring and of deformity in the eyebrow line. 2, 7
The dermatologic surgeon must recognize the various types of cutaneous flaps since there is a growing incidence of nasal tumors. Thus, the authors present an interesting method for reconstruction of nasal defects using a pedicled frontal interpolated flap with excellent aesthetic results. l
1. Chiummariello S, Dessy LA, Buccheri EM, Gagliardi DN, Menichini G, Alfano C, et al. An approach to managing non-melanoma skin câncer of the nose with mucosal invasion: our experience. Acta Oto-Laryngologica, 2008;128(8):915-9.
2. Padoveze EH, Cernea SS. Reconstrução dos defeitos nasais após exérese de tumores pela cirurgia micrográfica de Mohs. Surg Cosmet Dermatol, 2013;5(2):116-120.
3. Snow SN. Rotation flaps to reconstruct nasal tip defects following Mohs surgery. Dermatol Surg. 1997;23(10):916-9.
4. Laitano FF, Teixeira LF, Siqueira EJ, Alvarez GS, Martins PDE, Oliveira MP. Uso de retalho cutâneo para reconstrução nasal após ressecção neoplásica. Rev Bras Cir Plast. 2012;27(2):217-22.
5. Quintella MGM, Rosa IP, Enokihara MY, Hirata SH. Reconstrução da ponta nasal por retalho de pedículo miocutâneo unilateral. Surg Cosmet Dermatol. 2010;2(1):60-2.
6. Lima BS, Abdalla SC, Accioli Vasconcellos ZA, Accioli Vasconcellos JJ, Vieira VJ, Bins-Ely J, d'Éça Neves, R. Reconstrução nasal com retalho frontal: nossa experiência. ACM Arq Catarin Med. 2007;36(1):103-5.
7. Laureano Filho JR, Lago CAP, Silva PF, Santos LAM, Gonçalves FLN. Reconstrução nasal parcial com retalho frontal oblíquo: relato de caso. Rev Cir Traumatol Buco-Maxilar-Fac.2011;11(3):55-60.
The present study was carried out at the Fundação Alfredo da Matta - Manaus (AM), Brazil.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}