


Claudia Maria Duarte de Sá Guimarães
Keywords: LASERS; LASERS, SOLID-STATE; ONYCHOMYCOSIS; PHOTOTHERAPY;SPECTRUM ANALYSIS; TRICHOPHYTON.
Onychomycosis is a pathology that is responsible for over 50% of the diseases that affect the nails.1 Despite the treatment advances that have taken place with the introduction of antifungal drugs in the 1990s, its treatment remains a challenge.2
Onychomycosis in the halluces is difficult to treat and prone to recurrences. Dermatophyte fungi, non-dermatophyte fungi, and Candida spp3 constitute its primary causes. Some factors pertaining to the host have an influence on the treatment - age, gender, vascular disease, diabetes, hypertension, number of infected toenails, duration of infection, history of previous treatment, type of onychomycosis, percentage of involvement of the nail, nail thickness, presence of dermatophytoma, involvement of the matrix, lateral involvement, and growth rate of the nail.3 Other mentioned factors are inadequate hygiene, frequent trauma to the nail, athlete'sfoot, prolonged hydration of the skin, excessive sweating of the feet, a habit of walking barefoot, use of open-toed shoes, frequent swimming, the sharing of bathing facilities, and warm weather.4 The evaluation of these factors helps to guide treatment and indicates the need for combined therapies. In particular, it is possible to observe the increase of microorganisms such as Candida (albicans and parapsilosis) and Fusarium spp, in immunocompromised individuals.
The 1,064nm Nd:YAG laser lies in the vibrational spectroscopy range of the near infrared (NIR), corresponding to a 750 to 2,500nm wavelength. According to the physical characteristics of that range (studied through analytical methods), it is fast (one minute or less), non-destructive, non-invasive, promotes a high penetration of the radiation beam, is suitable for universal use.5, 6 The use of devices that emit NIR wavelengths has caused the photoinactivation of fungi and other microbial pathogens without damaging adjacent healthy tissues. The hypothesized action on the microorganisms is that of the interaction of the plasma and mitochondrial membranes, with the generation of oxygen radicals and the destruction of Staphylococcus aureus, Escherichia coli, Candida albicans and Trichophyton rubrum, among others.7, 8
A monocentric, retrospective, non-comparative clinical open study was conducted at a private practice in Rio de Janeiro, Brazil, to assess the effectiveness of 1,064nm sub-millisecond (0.3ms) Nd:YAG in the treatment of chronic onychomycosis. The study was conducted according to the ethical principles of the Helsinki Declaration of 1975, updated in 2000 and revised in Edinburgh in 2008.
Of the ninety-seven cases followed up, 30 patients were included. The study group consisted of individuals aged between 25 and 80 years, who bore onychomycosis in the right and/or left hallux - of mild, moderate, or severe intensity - for more than 3 years, and had undergone systemic and/or topical treatment for over a year without clinical improvement. The volunteers signed a free and informed consent term after receiving information about the disease and preventive care. Patients with a negative culture, use of systemic medication for less than one year, and who did not complete the course of treatment were excluded. The recommendations made to participants were: to use antifungal powder in the shoes (2mg undecylenic acid, 150mg zinc undecylenate, 60mg calcium propionate, 0.5mg hexylresorcinol), to wash socks in hot water, and to avoid using scissors to remove cuticles and trim nails (replacing the latter with disposable nail files).
Standardized photographs for clinical control were taken with a CanonT1i camera, 60mm fixed lens, flash, and white background. After collecting material for a culture, the 1,064nm Nd:YAG laser Joule (Sciton) was applied with a ClearSense handpiece at between 42-44ºC, in spiral movements on the external border towards the center of the nail. Energy was set at 5-7j/cm2, pulse duration at 0.3ms and repetition rate at 4.0Hz in three initial sessions at weekly intervals. The initial sessions were followed by further sessions up until the diseased nail had completely grown.
Patients with less than 50% involvement of the nail were followed up with every three months while those with more than 50% were seen monthly.
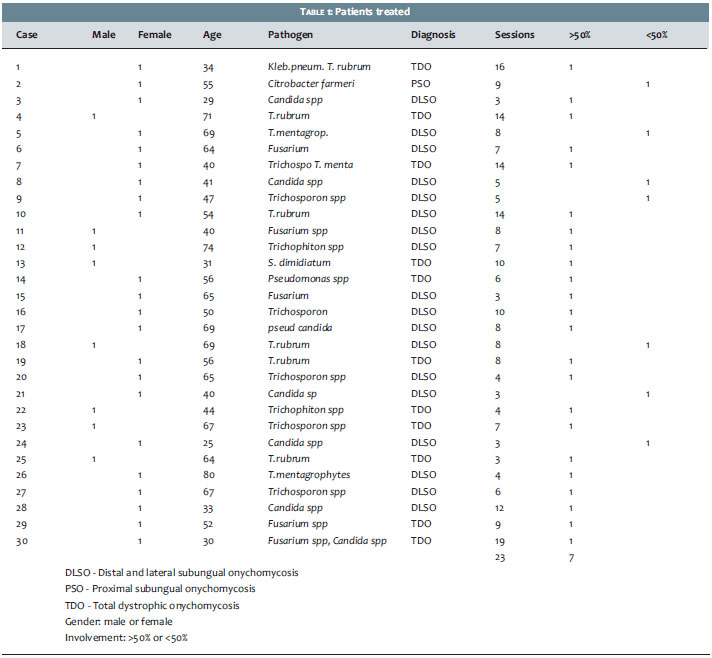
The treatment was well tolerated by patients, who showed only transient discomfort during laser application. No adverse effects were observed. The treatment duration and the number of sessions required were influenced by the intensity of involvement of the nail plate (Table 1). Of the 30 included patients, 18 were more than 50 years of age and 12 were younger than 50 years of age (6 were under 35 years of age). The involvement of the nail plate was greater than 50% in 23 cases and less than 50% in 7 cases. Pathogens found were Trichophyton mentagrophytes (4 cases), Trichophyton rubrum (5 cases), Trichosporon spp (8 cases), Candida spp (7 cases), Fusarium spp (5 cases), Scytalidium dimidiatum (1 case), and mixed infections (4 cases of association of fungi and/or bacteria). The number of sessions ranged from 3 to 16 for each case. Variable clinical improvement was observed in the treated nails. (Figures 1 to 5)
Light has been used since ancient times to treat diseases. The first experiments with phototherapy date back 100 years, when Raab and Von Tappeiner studied the action of red acridine on the culture of paramecium.
Since then, several types of dyes (including toluidine blue, methylene blue, eosin, 5-ALA etc), were tested in the elimination of microorganisms through photodynamic therapy.
However, some of the dyes used have considerable toxicity, and the absorption by the target requires the removal of the nail plate, hindering its clinical use. Currently, with the gradual increase of resistance of microorganisms to medications, other treatment methods, such as tests with less toxic dyes and the use of lasers in the NIR range (870/930nm, 1,064nm, 1,444nm), are being studied with the objective of destroying pathogenic fungi and bacteria with a minimum of damage to the host.
Onychomycosis is a difficult to treat disease that is influenced by factors pertaining to the host and the pathogen. The penetration of topical medications in the affected nail bed can be increased with the abrasion of the nail9 or with the use of strategies to improve the permeation of the drug through the use of sulphites, hydrogen peroxide, urea, and salicylic acid, among others.10 Among the substances mentioned, hydrogen peroxide and urea - in addition to the abrasion of the affected nail - are allies in the fight against dermatophytomas and very thick nails. The slow growth of nails due to the use of tight shoes or circulatory problems can be approached with guidance on the use of appropriate footwear, hygiene, and stimulation from a 1,064nm Nd:YAG laser.
The 1,064nm Nd:YAG laser, applied with low energy levels and short duration pulses, promotes angiogenesis, stimulates the production of collagen fibers11, 12 and promotes the alteration of the microorganisms' walls. Furthermore, it improves microcirculation of the extremities, accelerates nail growth and inhibits the multiplication of microorganisms without the inconvenience of the mutagenic effect of ultraviolet light. There is also the added advantage of not needing the use of photosensitizers - such as in photodynamic therapy, which combines the LED light (light-emitting diodes) in the NIR range.13-14
Carney et al., resting on the assumption that the effect of Nd:YAG laser could be due to the thermal effect or direct action of the viability of fungi, conducted a study to evaluate in vitro and in vivo three different pathogens - Trichophyton rubrum, Epidermophyton floccosum, and Scytalidium dimidiatum. The authors observed clinical improvement of 10 studied patients for 24 weeks, however could not confirm whether the action of hyperthermia would be sufficient to explain the reduced intensity of onychomycosis in the nails treated.
They used an energy level of 16 J/cm2, a pulse duration of 0.3 milliseconds, a spot size of 5mm and a repetition rate of 2.0Hz (500 shots per session on the ten nails) in all sessions, and have considered that the treatment caused pain and a burning sensation.15-21
In the experience of the author of the present article, the use of 5-7 J/cm2, pulse duration of 0.3 milliseconds, a 6mm spot size and a repetition rate of 4.0Hz are well tolerated, in several passes. Using the measurement of the handpiece's thermometer as the end point for the session, with enough accumulated energy to reach between 42-44ºC (indicated by the yellow light), it is possible to reach a higher number of shots (between 1,200 - 1,600) in the 10 nails treated. Real time temperature control is important to avoid onycholysis due to the coagulation of proteins, which happens at temperatures close to 50ºC.
The treatment of onychomycosis with 1,064nm Nd:YAG proved to be well tolerated. The treated cases showed acceleration of nail growth and improvement of the clinical aspect of the nails. Taking into consideration that only chronic cases already treated with other therapeutic modalities were selected, it can be stated that the use of the laser in question is an option valid for cases of treatment failure or those for which systemic medication is contraindicated.
1. Ghannoum MA, Hajjeh RA, Scher R, Konnikov N, Gupta AK, Summerbell R, et al. A large-scale North American Study of fungal isolates from nails: The frequency of onychomycosis, fungal distribuition, and anti-fungal susceptibility patterns. J Am Acad Dermatol. 2000;43(4):641-8.
2. Sigurgeirsson B. Prognostic factors for cure following treatment of onychomycosis. J Eur Acad Dermatol Venerol. 2010;24(6):679-84.
3. Scher RK, Tavakkol A, Sigurgeirsson B, Hay RJ, Joseph WS, Tosti A, et al. Onychomycosis: Diagnosis and definition of cure. J Am Acad Dermatol. 2007;56(6):939-44.
4. Nucci M, Anaissie E. Fusarium infections in immunocompromised patients. Clin Microbiol Rev. 2007;20(4):695-704.
5. Pasquini C. Near Infrared Spectroscopy:fundamentals, practical aspects and analytical applications. J Braz Chem Soc. 2003;14(2):198-219.
6. Knappe V, Frank F, Rohde E. Principles of lasers and biophotonic effects. Photomed. Photomed Laser Surg. 2004;22(5):411-7.
7. Landsman AS1, Robbins AH, Angelini PF, Wu CC, Cook J, Oster M, et al. Treatment of mild, moderate, severe Onychomycosis using 870 and 930nm light exposure. J Am Podiatr Med Assoc. 2010;100(3):166-77.
8. Gonçalves F, Zanetti AL, Zanetti RV, Ramalho SA. Estudo in vitro do laser de diodo 980nm na desinfecção de implantes. RGO (Porto Alegre). 2009;57(4):395-9.
9. Chiacchio N Di, Kadunc BV, Almeida ART, Madeira CL. Nail abrasion. J Cosmet Dermatol. 2004;2(3-4):150-2.
10. Shivakumar HN, Juluri A, Desai BG, Murthy SN. Ungual and Transugual drug delivery. Drug Develop Indust Pharm. 2012;38(8):901-11.
11. Dayan SH, Vartanian AJ, Menaker G, Mobley SR, Dayan AN. Nonablative laser resurfacing using the lon-pulse (1064nm) Nd:YAG laser. Arch Facial Plast Surg. 2003;5(4):310-5.
12. Dayan S, Damrose JF, Bhattacharyya TK, Mobley SR, Patel MK, O'Grady K, et al. Histological evaluations following 1,064nm Nd:YAG laser resurfacing. Lasers Surg. Med. 2003;33(2):126-31.
13. Waibel J, Jared A WBS, Rudnick A. Prospective efficacy and safety evaluation of laser treatments with real-time temperature feedback for fungal onychomycosis. J Drugs Dermatol. 2013;12(11):1237-42.
14. Ledon JA, Savas J, Franca K, Chacon A, Nouri K. Laser and light therapy for onychomycosis: a systematic review. Lasers Med Sci. 2014;29(2):823-9.
15. Bornstein E. A review of current research in light-based Technologies for treatment of podiatric infections disease states. J Am Podiatr Med Assoc. 2009;99(4):348-52.
16. Vural E, Winfield HL, Shingleton AW, Horn TD, Shafirstein G. The effects of laser irradiation on Trichophyton rubrum growth. Lasers Med Sci 2008;23(4):349-53.
17. Meral G, Tasar F, Kocagöz S, Sener C. Factors affecting the antibacterial effects of Nd-YAG laser in vivo. Lasers Surg Med. 2003;32(3):197-202.
18. Kimura U1, Takeuchi K, Kinoshita A, Takamori K, Hiruma M, Suga Y. Treating onychomycosis of the toenail: clinical efficacy of the sub-millisecond 1,064nm Nd:YAG laser using a 5mm spot diameter. J Drugs Dermatol 2012. 2012;11(4):496-504.
19. Hochman LG. Laser treatment of onychomychosis using a novel 0,65-milisecond pulsed Nd:YAG-nm laser. J Cosmet Laser Ther. 2011;13(1):2-5.
20. Naouri M, Mazer JM. Traitment d'une onychomycose digitale à Candida tropicalis par laser Nd:YAG short pulse. Ann Dermatol Venereol. 2013;140(10):610-3.
21. Carney C, Cantrell W, Warner J, Elewski B. Treatment of onychomycosis using a submillisecond 1064-nm neodymium:yttrium-aluminum-garnet laser. J Am Acad Dermatol. 2013;69(4):578-82.
The present study was carried out in the author's private practice - Rio de Janeiro (RJ), Brazil.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}