


Guilherme Bueno de Oliveira1; Natalia Cristina Pires Rossi2; Doramarcia de Oliveira Cury2; Julia Maria Avelino Ballavenuto3; Carlos Roberto Antonio4; João Roberto Antonio5
Keywords: NAIL DISEASES; NAILS; NAIL BITING.
The transverse over-curvature of the nail is clinically classifiedinto three types: 1) Pincer nail - where the over-curvature is increased along the axis in the proximal to distal direction (most common); 2) Tile nail - where there is a transverse over-curvature, however with the lateral margins remaining parallel; and 3) Folded nail - where there is moderate convexity on one or both sides of the lateral margins, which abruptly changes the angle, piercing in a cutting manner, on the lateral portion of the nail bed.1-3
The pincer nail most commonly affects the toes, occurring rarely in the fingers. 2, 3 Its etiology has not yet been fully elucidated, being attributed to several factors and diseases. As it evolves, the over-curvature can cause pain, discomfort when using closed shoes, and secondary infections.3-5
Several surgical techniques have been proposed to correct deformities of the nail, varying according to the purpose of the treatment.6-8 Although not having yet been enshrined in the technical literature, Fanti's technique is an alternative proposed for the treatment of pincer nails.
Eleven patients with pincer nails were selected from the Hair and Nails Ambulatory of the Dermatologic Clinic of the The Faculdade de Medicina Estadual de São José do Rio Preto São José do Rio Preto (SP), Brasil. All patients underwent surgical and radiological evaluation with X-ray before undergoing surgery. The study was conducted according to the norms established by the Declaration of Helsinki 2000.
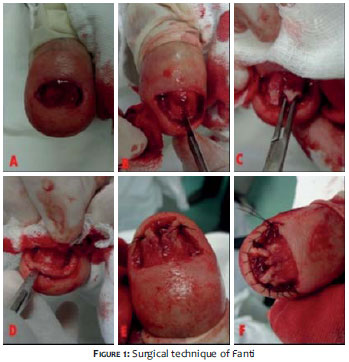
The goal of the surgical Fanti's technique is to widen the nail bed, decreasing the existing constriction. The complete technique consists of the following steps: 1) Asepsis of the finger; 2) Nerve block anesthesia with 2% lidocaine without epinephrine; 3) Placement of the tourniquet; 4) Total removal of the nail plate (Figure 1A); 5) Phenolization of the nail matrix (bilateral); 6) Median longitudinal incision of the nail bed up to the bone plane - from the free border up to the point just before the lunula - and excision in a "U" shape of the lateral and distal borders (Figures 1B, 1C and 1D); 7) Detachment of the nail bed close to the bone, creating two flaps; 8) Osteotomy of the ventral surface of the distal phalanx if necessary and diagnosed in the radiological evaluation (Figure 2); 9) Suture of the flap's tip with 4-0 monofilament nylon thread, laterally, in the nail fold (Figure 1D); 10) Hemostatic running sutures in the lateral and distal folds with 4-0 monofilament nylon thread (Figure 1F); 11) Removal of the tourniquet; 12) Application of dressing. The dressing is kept for 48 hours and then changed daily. The stitches are removed within 7 to 14 days.
Patients undergoing Fanti's technique surgery had a thickened nail plate, clamping all along the longitudinal axis, mainly distal, and atrophy with keratinization of the nail bed. (Figures 3 and 4) After 14 months of observation there was significant improvement in the function of the nail, with an absence of symptoms and normalization of the local appearance, rectification of the nail plate and lengthening of the bed (Figures 5 and 6).
Post-operatively, all patients had moderate pain for a week, being more intense in the first 24 hours. After the removal of the stitches (7 to 14 days after the surgery), there were no reports of pain. The removal is allowed when the aspect of the nail is that of an adherent hematic crust (Figure 7).
The nail's function and aesthetics begin 21 days after the procedure and become complete in three months. In the third week, patients were allowed to use closed shoes with dressings dampened with oils, with an absence of reports of pain.
Pincer nails can be inherited or acquired. The hereditary type, where family history and symmetry are present, usually affects the hallux but can affect any of the other toes or fingers.1, 2, 6 The acquired type, where a main feature is the asymmetry, can be further subdivided into: a) secondary to orthopedic defect (when it is often caused by the deviation of phalanges due to the use of tight or inadequate shoes; b) secondary to chronic dermatoses (such as psoriasis, subungual exostosis, epidermal and myxoid cyst, onychomycosis, implantation of arteriovenous fistulas in the forearm - hemodialysis, medications - beta-blockers, association with metastatic adenocarcinoma of the sigmoid colon - marker, Kawasaki's disease, or the association with epidermolysis bullosa simplex; c) secondary to degenerative osteoarthritis of the distal interphalangeal joint of the fingers.2, 3 The congenital pachyonychia has a differential diagnosis with the pincer nail, being distinguished from the latter by not usually causing pain and by affecting the fingers and toes.3
In order to perform the surgical treatment, the main indications are for patients suffering from pain and inflammation. Patients who have already undergone conservative treatment without success also provide indications for the procedure. Another major complaint reported by patients is the loss of quality of life: there is aesthetic embarrassment, in addition to the limitation of the use of certain types of footwear, mainly the closed type.4, 6, 7
Many surgical techniques have been reported in the literature for the treatment of pincer nails.8 The most important options for the surgical treatment of over-curvature, are those with techniques aimed at reducing the width of the matrix and the proximal nail plate: the phenolization of the lateral overcurved horns, which eliminates the pain caused by the clamping of the bed, thus bringing immediate improvement to the pain; the technique described by Haneke, which combines the phenolization with the median incision of the nail bed; the detachment, which reduces the traction of the periosteum on the same; the removal of osteophytes, if required; and the reverse suture, seeking the rectification of the nail bed.3, 6, 7
The present work demonstrates the surgical Fanti's technique for the correction of pincer nails, where the anatomical and functional improvement of the operated nail can be observed.
1. Zook EG1, Chalekson CP, Brown RE, Neumeister MW. Correction of pincer-nail deformities with autograft or homograft dermis:modified surgical technique. J Hand Surg. 2005;30(2):400-3.
2. Richert B, Di Chicchio N, Haneke E. Cirurgia da unha. Rio de Janeiro: Di Livros; 2012.
3. Baran R, Haneke E, Richert B. Pincer nails: definition and surgical treatment. Dermatol Surg. 2001;27(3):261-6.
4. Plusjé LG. Pincer Nails: a new surgical treatment. Dermatol Surg. 2001;27(1):41-3.
5. Tosti A, Piraccini BM, Di Chiacchio N. Doenças das Unhas. São Paulo: Editora Luana; 2007.
6. Tavares GT, Di Chiacchio N, Loureiro WR, Di Chiacchio NG, Bet dl. Correção de hipercurvatura transversa da unha utilizando enxerto de derme autóloga. Surg Cosmet Dermatol. 2011;3(2):160-2.
7. Tassara G, PINTO JM, Gualberto GV, Ribeiro BS. Tratamento de unha em telha pela técnica de Zook: relato de cinco casos. An Bras Dermatol 2008;83(3): 83-6.
8. Di Chiacchio NG, Ferreira FR, Mandelbaum SH, Di Chiacchio N, Haneke E. Cirurgia das unhas. Seguimento de casos operados em curso prático realizado em Congresso Dermatológico. Surg Cosmet Dermatol 2013;5(2):134-¬6.
The present study was carried out at the Faculdade de Medicina Estadual de São José do Rio Preto (FAMERP) - São José do Rio Preto (SP), Brazil.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}