


Elisa de Oliveira Barcaui1; Antonio Carlos Pires Carvalho2; Juan Piñeiro-Maceira3; Paulo Marcos Valiante4; Carlos B Barcaui5
Keywords: ULTRASONOGRAPHY; SKIN NEOPLASMS; DIAGNOSIS.
The skin is an extensive organ that, due to its function as a surface covering for the body, enables the performance of noninvasive diagnostic and investigative procedures. With the increasing incidence of malignant neoplasias (melanoma and non-melanoma), especially in relatively young individuals, it has become a challenge to establish correct diagnoses that serve to identify malignant lesions, eliminate unnecessary surgical procedures, and minimize unsightly problems arising from therapeutic approaches. Within this context, new methods of imaging for diagnosis have been developed. Techniques such as dermoscopy, confocal microscopy, and high frequency ultrasound (HFUS) enable the real-time study of cutaneous lesions, making them excellent pre-operative tools. However, these methods vary considerably as far as their penetration, resolution, and applicability are concerned. Dermoscopy is a complementary exam of great impact in dermatological practice, allowing early differentiation of benign and malignant cutaneous lesions. With this resource, it is possible to assess the extent of a lesion in its longitudinal and transverse axes. It is impractical, however, for determining the depth and possible invasion of adjacent structures such as cartilage and muscle, based solely on clinical-dermoscopic evaluation.
The recent development of ultrasound devices with a frequency greater than 15MHz have made it possible to identify the skin's different layers, structures, and appendages, thus considerably expanding the use of this technology in the investigation of dermatologic lesions. HFUS allows for the delimiting of the margins of the neoplasia, due to the difference in echogenicity between the hypoechoic tumoral area and the hyperechoic perilesional area.
Used in tandem, Color Doppler examination allows the assessment of a tumor's vascularization, nature, and distribution. In this way, HFUS facilitates the study of cutaneous neoplasms, due to the fact that it recognizes the lesion, provides its exact size, location, and vascular pattern, in addition to identifying involved cutaneous layers and adjacent structures, all in a noninvasive manner.
The incidence of cutaneous malignant neoplasias - melanoma and non-melanoma - has been increasing steadily in recent years. The precise statistics related to this development are difficult to determine due to varying data records, structures, and data acquisition protocols.1, 2
Of all the tumors that affect humans, non-melanoma cutaneous cancer is the most common.3 Most of the neoplasias of this type are derived from alterations in the skin's basal and squamous cells, resulting in basal cell carcinoma (BCC) and squamous cell carcinoma (SCC), respectively. Malignant lesions originating from other cell types present in the cutaneous structure, such as Merkel cells, lymphocytes, vascular endothelial cells, cell forming adnexal structures and mesenchymal stromal cells, can also be classified as non-melanoma skin cancer. However, due to their low frequency, the present study will only cover BCC and SCC.4
It is estimated that the incidence of BCC - in its isolated form - has been increasing 10% annually, on a universal basis. 1 In Brazil, according to the National Cancer Institute (INCA), 63,280 new cases were diagnosed in 2012.5
Melanoma is the most aggressive tumor occurring in the human species. Its incidence has grown more than that of any other solid tumor in recent decades.6 It is estimated that 200,000 new cases and 48,000 deaths resulting from this neoplasia occur worldwide every year.2 The best current strategy to reduce the death rate is early diagnosis.7
Basal Cell Carcinoma
BCC is the most common cutaneous neoplasia (75-90%).
Approximately 40% of patients diagnosed with BCC will present one or more lesions belonging in that category in the subsequent 10 years.8 Statistically, 80% of cases occur in people over 60 years old.1 Epidemiological studies however, show that its incidence has been increasing drastically in younger individuals.4 Factors such as a predilection for having body areas exposed to the sun, and the higher prevalence in countries near the Equator, confirm the role of solar radiation in tumoral genesis. Intense and intermittent exposure to the sun, particularly during childhood and adolescence, increases the risk of the disease.1 Immunosuppression also predisposes BCC. In immunocompetent individuals, the BCC to SCC ratio is 4:1, whereas in transplanted patients that ratio is inverted. The mutation of the tumor suppressor genes p53 and PTCH (hedgehog signaling pathway) can be found in BCC cases.9
Clinically, recent lesions are small, translucid or pearly, with telangiectasias. They do not have precursor lesions. The most common subtypes are: nodular, superficial, pigmented, ulcerated, and morpheaform. The nodular type is the most frequent and is located preferentially in the head and neck. The nodule grows slowly and may undergo central ulceration. The superficial type consists of a plaque with peripheral growth and occurs predominantly in the trunk. The pigmented type, owing to the fact that it contains melanin, must be differentiated from melanoma. Due to the fact that it has imprecise limits, the morpheaform type can be difficult to diagnose clinically.8, 9
Regarding the histopathological classification, the World Health Organization (WHO) suggests that subtypes be differentiated according to the growth pattern: nodular (solid, adenoid and cystic), superficial, micronodular, and infiltrative.
Due to the high recurrence rate, the last three sub-types are considered high risk.8 The association of two or more histopathological subtypes is common in the same lesion, (10-40% of cases).1
BCC grows through direct invasion and appears to require that the adjacent stroma support its growth, which would explain its low capacity for metastasizing through blood and lymphatic vessels.10 When they occur, metastases are derived from primary tumors located typically on the face and ear, and affect regional lymph nodes, bones, lungs, and liver.9
Studies indicate a high rate of recurrence for lesions located on the face (mainly on the eyelids, nose, and ears) and those that were incompletely excised at an earlier time.11 As a result, therapeutic measures - such as wide surgical resection, which can lead to functional and aesthetic problems - are often adopted. On the other hand, incomplete excisions are to blame for changes in the structure of tumors, which cause a more aggressive behavior.12, 13
Sartore et al. suggest that 5-50% of BCCs are incompletely excised.10 The determination of the tumor's extension and correct safety margin is instrumental when selecting the therapeutic choice, as the ultimate goal is the complete elimination of the tumor with maximum preservation of function and aesthetics. 9, 10
Squamous Cell Carcinoma
Originating in the epithelial cells of the skin and mucosa, SCC has the capacity for local invasion and metastasizing from a distance. In accordance with their malignant potential, SCCs are frequently classified into two groups: those originating from skin with actinic damage (less aggressive, metastasizing in less than 1% of cases) and those originating from areas of ionizing and non-ionizing radiation, chronic fistulae tracts, and areas of burns or chronic ulcers (typically more aggressive).
Etiopathogenic factors are similar to those of BCC. Immunosupression - both in transplanted patients and in those undergoing phototherapy for long periods - significantly increases the risk of developing SCC. In such cases, the disease is more aggressive. Human papillomavirus types 16 and 18 are found in squamous neoplasias in the genital area. Arsenic can be responsible for in situ and invasive lesions.1, 14
Lesions on the genitalia, mucosa, and ears that are greater than 2cm in size and located in sites of chronic inflammation, such as burn scars, have a higher risk of metastasizing.1, 15
The initial lesion, both in healthy skin and in that affected by a pre-malignant disease, appears as a papule, nodule, or redish plaque, in general keratotic or ulcerated. SCC has rapid growth when compared to BCC. In Caucasians, the main location is in body areas exposed to the sun, while in dark-skinned individuals it most commonly arises in the lower limbs (trauma). As in most cases SCC metastasizes first to regional lymph nodes, thus the latter should be always examined in the presence of a clinically suspected lesion.16
Melanoma
Originating from melanocytes, melanoma in general arises in primary cutaneous sites. Nevertheless it can occasionally occur in the eyeball, meninges, and mucous membranes. It affects both genders.
The prevalence is higher in fair-skinned individuals, in bearers of dysplastic nevus syndrome, and in patients with more than 50 melanocytic nevi.2, 6
The risk of developing melanoma depends on genetic and environmental factors. Although pathogenic mechanisms are not fully understood, genetic factors such as mutations of the gene MC1R associated with environmental factors, especially exposure to the sun, predisposes individuals to the disease. The mutation of the gene CDKN2A is present in cases of familial melanoma and in patients with multiple melanoma. Although rare, the mutation of the gene CDK4 substantially increases susceptibility to the disease.6
The manner in which patients undergo exposure to the sun affects the clinical course of melanoma: intense intermittent exposure on the trunk of patients with multiple nevi is associated with the disease in middle-aged individuals (there is a correlation with the mutation of BRAF), while in elderly individuals, the association is made with chronic exposure to the sun. Alterations in the immune system also precipitate the genesis of melanoma: congenital or acquired immunodeficiency and immunosuppression (chemotherapy for neoplasias or in transplanted patients) are associated with multiple or metastatic lesions. Melanoma can develop from a preexisting nevus lesion (20 to 40% of cases) or de novo.2
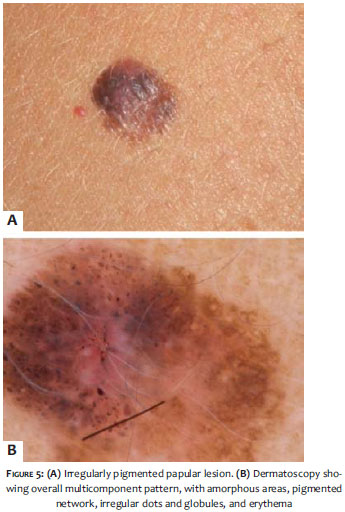
Clinically and pathologically, melanoma can be classified into: superficial extensive, nodular, lentigo maligna, and acral. The extensive superficial type corresponds to 70% of cases and often affects the trunk in men and the lower limbs in women. From a clinical point of view, the lesions are maculopapular with different hues. The nodular type of melanoma has a hemispheric appearance - pedunculated or not. The lentigo maligna type has a better prognosis and its incidence increases with age, influenced by exposure to the sun. The acral type of melanoma is more frequent in dark-skinned individuals. In general it has a late diagnosis, which results in a worse prognosis.6
Regardless of its clinical form, the lesion is characterized as being asymmetric and having irregular borders, varied colors, and a diameter in excess of 6mm, all of which adheres to the ABCD rule. Despite presenting well-established criteria for the clinical/morphological diagnosis, one in every three cases is diagnosed incorrectly.17
Used in dermatology since the 1970s, ultrasonography is a painless non-radioactive imaging diagnostic method based on the reflection of sound waves through body tissues.12, 18 According to the anatomical structure, vascularization, and density, ultrasonic waves are reflected back to the transducer, which turns them into a grayscale that can be observed on a screen. The images are visualized through vertical sections.19
The higher the frequency of the waves emitted by the transducer, the greater the spatial resolution and resulting visualization of the structures close to them. The introduction of transducers with a frequency greater than 15MHz has originated the high frequency ultrasound (HFUS). The shorter wavelength obtained with this frequency allows better evaluation of superficial structures, significantly expanding its use in skin conditions.20
Equipment with frequencies above 15MHz facilitates studying the skin and its annexes because it makes it possible to distinguish the skin's layers and structures. However, equipment with frequencies above 20MHz has better resolution for studying the superficial structures.21
In the cutaneous ultrasound analysis, it is recommended that a thick layer of gel be used between the skin and the transducer in order to obtain a better focal point.12
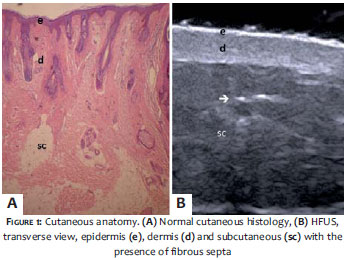
It is important to use a sensitive transducer, which adapts to the cutaneous contour of the different body regions, such as the face and distal phalanx. Contact between the transducer and the skin should be as gentle as possible, avoiding the compression of anatomical structures, which are superficial and thin in this tissue. In normal skin, the echogenicity of each layer depends on its respective main component, which is the keratin in the epidermis, collagen in the dermis, and fat lobules in the subcutaneous tissue.
In ultrasound imaging, the epidermis appears as a hyper-echoic line, the dermis as a hyperechoic band (not as smooth as the epidermis), and the subcutaneous layer as a hypoechoic layer (with the presence of hyperechoic fibrous septa within).18 (Figure 1)
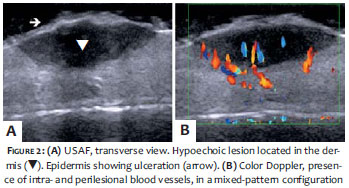
Under ultrasound, cutaneous neoplasms usually present as homogeneous hypoechoic areas contrasting with the adjacent healthy tissue.22 In addition to the echogenicity, it is possible to measure the borders longitudinally, transversely, and axially, as well as the contour and the involvement of deep layers such as muscles, cartilage, and bones. The study of vascularization can be carried out in combination with the assistance of a Color Doppler or PowerDoppler, which allows the observation of the type, size, and nature (arterial or venous) of the tumor's vessels.12 (Figure 2)
As cutaneous lesions can be asymmetric, the measurement of tumor thickness must be based on the location of greatest invasion.23
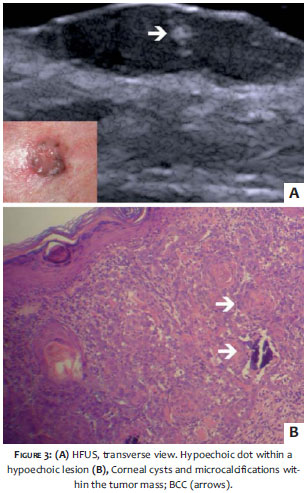
Under HFUS, BCC appears as a well-defined hypoechogenic area with irregular contour, usually located in the dermis - nevertheless it can reach deeper planes.11
The presence of hyperechoic spots can often be observed within the tumor. (Figure 3A) These images are attributed to the presence of corneal cysts, microcalcifications, or clusters of apoptotic cells within the tumor mass.22, 24 (Figure 3B) There are reports in the literature of subclinical satellite lesions that were diagnosed using HFUS.11 Intra- and peritumoral blood flow is minor, consisting of low-flow arteries and veins.12
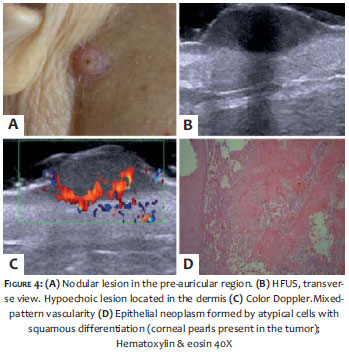
Although BCC and SCC are similar in appearance under HFUS, it is possible to distinguish between these two tumors, since the latter does not have the hyperechoic spots within the neoplasm. Due to SCC's more aggressive behavior, is more likely to invade adjacent soft tissues, cartilage, and bones. Color Doppler based mapping displays a mixed pattern, with internal and peripheral vascularization (Figure 4). Marmur et al. point out that due to the fact that SCC generally presents hyperkeratosis and has a greater associated inflammatory process, the tumoral area can be overestimated when assessed with ultrasound.22
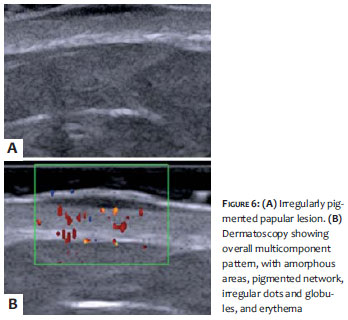
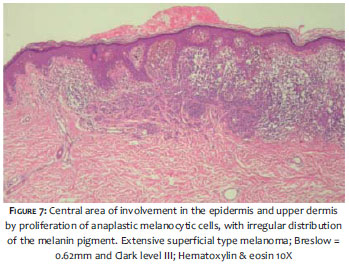
With melanoma, HFUS is used to establish the tumoral thickness, margins, and vascularization. Nevertheless, although nevus lesions present irregular echogenicity (while the appearance of melanoma is homogeneous), these lesions cannot be differentiated under HFUS, which may overestimate the tumor's size.7, 25, 26 (Figure 5) In an ultrasound image, melanoma usually appears as a homogeneous hypoechoic area, oval or fusiform in shape.27 (Figures 6 and 7) In ulcerated lesions, the epidermis may be irregular.19 The mapping of melanocytic lesions with Color Doppler demonstrates that, in melanoma, vascularization is more intense than in benign lesions, with the predominance of low-flow arterial vessels. The metastatic potential of these lesions can be estimated by studying the angiogenesis.28, 29 The sonographic evaluation of involvement of regional lymph nodes shows better outcomes for detection of metastases than that of the clinical examination.23
Some factors may lead to errors in the measurement of tumoral thickness with HFUS; an inflammatory process associated with neoplasia, procedures prior to the examination, a presence of perilesional hypertrophic glands and association with nevus/melanoma can induce the overestimation of their size. On the other hand, the presence of ulceration can induce underestimation. As limitations of the method, the authors cite the inability to detect epidermal lesions and those with diameters less than 1mm, in addition to the fact that it is operator-dependent.10, 12, 21, 24
To date, histology is the gold standard for diagnosis and structural morphological evaluation of cutaneous neoplasms. However, new techniques for in vivo diagnosis have been used to streamline diagnosis and optimize pre-operative evaluation. HFUS examination exists as a great method to evaluate skin cancer. As it is incapable of assessing tumor cellularity, it cannot be used to confirm diagnosis. However it does allow for the performing of detailed pre-operative study, examination of the different skin layers and their respective thicknesses, indicating the tumor nature (cystic or solid), and providing their size, exact location and the involvement of adjacent structures.
In combination, the blood flow of the lesion and its surrounding area can be estimated by Color Doppler ultrasonography. This analysis provides important parameters for the guidance of the therapeutic approach.
1. Madan V, Lear JT, Szeimies RM. Non-melanoma skin cancer. Lancet. 2012;375(9715):673-85.
2. Eggermont AMM, Spatz A, Robert C. Cutaneous melanoma. Lancet. 2014;383(9919):816-27.
3. Diepgen TL, Mahler V. The epidemiology of skin cancer. Br J Dermatol. 2002;146(suppl 61):1-6.
4. Ridky TW. Nonmelanoma skin cancer. J Am Acad Dermatol. 2007;57(3):484-501.
5. INCA.org [Internet]. Rio de Janeiro: Instituto Nacional do Câncer José Alencar Gomes da Silva. [Acessado em 20 abril 2014]. Disponível em: http:// www2. INCA. gov.br/ wps/ wcm/ connect/ inca/portal/home
6. Négrier S, Fervers B, Bailly C, et al. Cutaneous melanoma. Br J Cancer. 2001;84(2):81-5.
7. Psaty EL, Halpern AC. Current and emerging technologies in melanoma diagnosis: the state of the art. Clin Dermatol. 2009;27(1):35-45.
8. Raasch BA, Buettner PG, Garbe C. Basal cell carcinoma: histological classification and body-site distribution. Br J Dermatol. 2006;155(2):401-7.
9. Rubin AI, Chen EH, Ratner DR. Basal cell carcinoma. N Engl J Med. 2005;353(21):2262-9.
10. Nassiri-Kashani M, Sadr B, Fanian F, Kamyab K, Noormohammadpour P, Shahshahani MM, et al. Pré-operative assessment of basal cell carcinoma dimensions using high frequency ultrasonography and its correlation with histopathology. Skin Res Technol. 2013;19(1):e132-e38.
11. Bobadilla F, Wortsman X, Muñoz C, Segovia L, Espinoza M, Jemec GB. Pré-surgical high resolution of facial basal cell carcinoma: Correlation with histology. Cancer Imaging. 2008;8:163-72.
12. Wortsman X. Sonography of facial cutaneous basal cell carcinoma. A first-line imaging technique. J Ultrasound Med. 2013;32(4):567-72.
13. Ochanha JP, Dias JT, Miot HA. Relapses and recurrences of basal cell carcinoma. An Bras Dermatol. 2011;86(2):386-9.
14. Stern RS, Liebman EJ, Vakeva L. Oral psoralen and ultraviolet-A light (PUVA) treatment of psoriasis and persistent risk of nonmelanoma skin cancer. PUVA Follow-up Study. J Natl Cancer Inst 1998;90(170:1278- 84.
15. Fitzpatrick PJ, Harwood AA. Acute epithelioma--an aggressive squamous cell carcinoma of the skin. Am J Clin Oncol. 1985;8(6):468-71.
16. Rieger KE, Linos E, Egbert BM, Swetter SM. Recurrence rates associated with incompletely excised low-risk nonmelanoma skin cancer. J Cutan Pathol. 2010;37(1):59-67.
17. Wolf IH, Smolle J, Soyer HP, Kerl H. Sensivity in the clinical diagnosis of Malignant melanoma. Melanoma Res. 1998;8(5):425-9.
18. Wortsman X, Wortsman J. Clinical usefulness of variable-frequency ultrasound in localized lesions of the skin. J Am Acad Dermatol. 62(2):247-56.
19. Ulrich M, Stockfleth E, Roewert-Huber J, Astner S. Noninvasive diagnostic tools for nonmelanoma skin cancer. Br J Dermatol. 2007;157(2):56-8.
20. Kleinerman R, Whang TB, Bard RL, Marmur ES. Ultrasound in dermatology: principles and applications. J Am Acad Dermatol. 2012;67(3):478-87.
21. Crisan M, Crisan D, Sannino G, Lupsor M, Badea R, Amzica F. Ultrasonographic staging of cutaneous malignant tumors: an ultrasonographic depth index. Arch Dermatol Res. 2013;305(4):305-313.
22. Marmur ES, Berkowitz EZ, Fuchs BS, Singer GK, Yoo JY. Use of high frequency, high resolution ultrasound before Mohs surgery. Dermatol Surg. 2010;36(6):841-847.
23. Wortsman X. Sonography of the primary cutaneous melanoma: a review. Radiol Res Pract. 2012;2012:814396.
24. Desai TD, Desai AD, Horowitz DC, Kartono F, Wahl T. The use of high-frequency ultrasound in the evaluation of superficial and nodular basal cell carcinoma. Dermatol Surg. 2007;33(10):1220-7.
25. Kaikaris V, Samsanavičius D, Kęstutis Maslauskas, Rimdeika R, Valiukevičienė S, Makštienė J, et al. Measurement of melanoma thickness - comparison of two methods: ultrasound versus morphology. J Plast Reconst Aesthet Surg. 2011;64(6):796-802.
26. Dummer W, Blaheta HJ, Bastian BC, Schenk T, Bröcker EV, Remy W. Preoperative characterization of pigmented skin lesions by epiluminescence microscopy and high-frequency ultrasound. Arch Dermatol. 1995;131(3):279-85.
27. Guitera P, Menzies SW. State of the art of diagnostic technologyfor earlystage melanoma. Expert Rev AnticancerTher. 2011;11(5):715-23.
28. Machet L, Belot V, Naouri M, Boka M, Mourtada Y, Giraudeau B, et al. Preoperative measurement of thickness of cutaneous melanoma using high-resolution 20 MHz ultrasound imaging: a monocenter prospective study and systematic review of the literature. Ultrasound Med Biol. 2009;35(9):1411-20.
29. Bessoud B, Lassau N, Koscielny S, Longvert C, Avril MF, Duvillard P, et al. High-frequency sonography and color doppler in the management of pigmented skin lesions. Ultrasound Med Biol. 2003;29(6):875-879.
The present study was carried out at the Department of Radiology, Universidade Federal do Rio de Janeiro (UFRJ) - Rio de Janeiro (RJ), Brazil.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}