


Luis Fernando Figueiredo Kopke
Keywords: BIOPSY; AMBULATORY SURGICAL PROCEDURES; MOHS SURGERY; PATHOLOGY, SURGICAL; SKIN NEOPLASMS.
In cutaneous oncology it is not uncommon to come across tumors with poor clinical demarcation-a situation that can hinder defining even the starting point for an excision.
Tumors with predominantly infiltrative growth may offer difficulties for their detection, especially in the early stages, when the clinical appearance is that of hypopigmented macules or slightly elevated plaque with poorly defined margins. These lesions arise mainly on the face of patients with fair and photo-damaged skin. In some cases, multiple procedures (curettage and eletrocauterization, cryotherapy, and even surgery), in addition to the use of topical medications (5-Fluorouracil, imiquimod and others), which can cause partial regression of tumors, can still compromise the determination of boundaries.
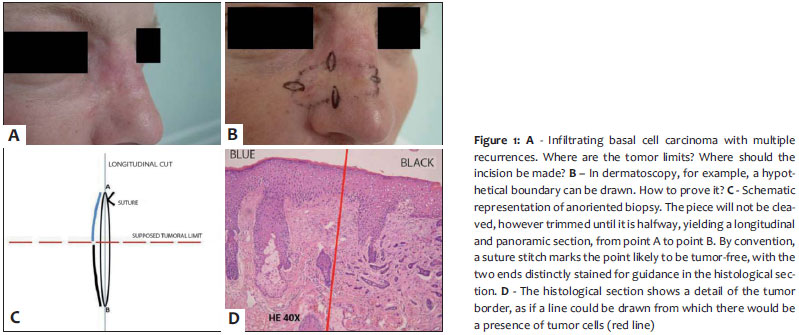
Although indistinguishable in those situations, a tumor's margin can be further examined through a topographically oriented, narrow fusiform excision, which can provide more comprehensive information and through which it is possible to view the tumor along a variable extent. This would be the theoretical conception of an oriented biopsy (Figure 1).
Depending on the size of the tumor and its predominant histologic type, the oriented biopsy may be incisional or excisional. Conceptually, nothing prevents the use of an oriented biopsy in tumors that are clinically well visible, however this technique is more useful in the evaluation of tumors with difficult clinical delimitation or that conflict from a histopathological point of view.
The extent and orientation of the fusiform excision will depend on the required or needed overview. In this way, it is possible to plan more than one fusiform excision in different orientations (one latero-lateral and another cranial-caudal, for instance). As for the longitudinal extension, it would be advisable that it did not exceed 2cm, as that could hinder its inclusion in the histological preparation, since ordinary microscope slides are 2.5cm wide. This however does not constitute a limiting factor, given that it is possible to prepare the slide in its longitudinal direction, enabling specimens of over 2.5cm long. However, from a practical standpoint, the maximum length of 2cm appears to be sufficient in most cases.
It is important that the ellipsis is not wide, but very thin, as this will facilitate the inclusion of the material. However, ellipses that are too thin may prove fragile and rupture during the laboratory process, which would undermine the purpose of such an examination.
Once the orientation of the fusiform excisions are established, a suture will be placed at one end to mark it-conventionally, by the side that is potentially tumor-free. A sketch of the entire topographical situation is drawn, instructing the laboratory to stain the ellipses' opposite sides in different colors, thus orienting the cut and the biopsy. Preferably, these details should be photographed, avoiding future difficulties of interpretation when the blades are finalized.
The laboratory must be familiar with the procedure, otherwise undue cuts and cleavages may occur. Cleaving the fragment should be avoided. It is easier and safer to include it in its entirety so that one of its sides is completely presented to the microtome knife. Preferably, the block should be trimmed in its longitudinal direction up to the point where the central regionbe reached. In this manner, it is possible to obtain an overview from one end to the other, distinctly stained.
Situations of applicability of the technique
1. Planning of the initial incision in cases of micrographic surgery, as already illustrated in Figure 1.
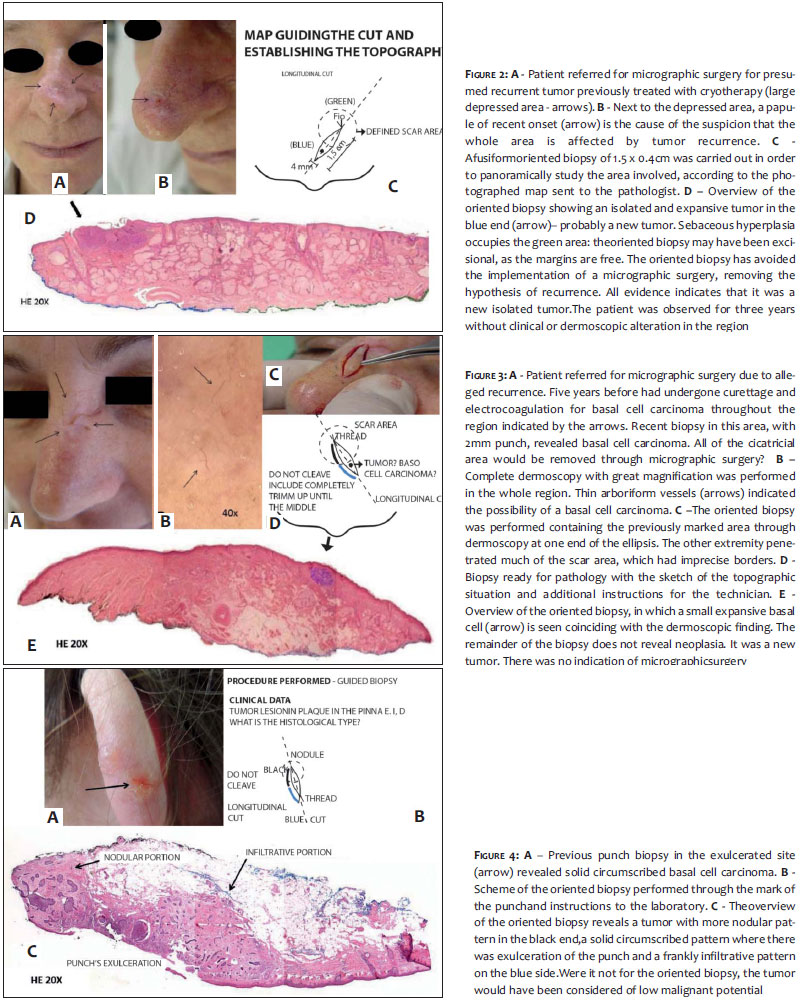
2. Collection of more reliable data than that provided by punctiform multiple biopsies, which may fail for lack of the panoramic view (Figures 2 to 4).
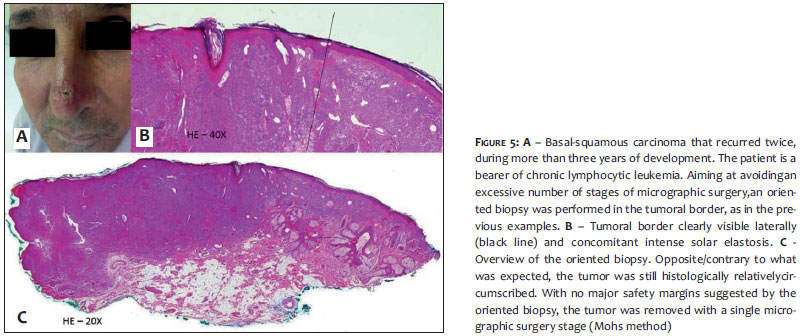
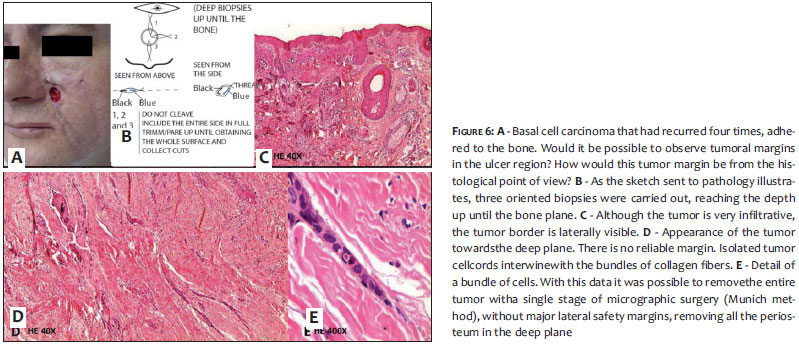
3. Complete study of the lateral and deep borders of the tumor (Figures 5 and 6).
Although no specific bibliographic reference on the subject in the literature has been found, one might intuitively think that this procedure is already routinely carried out, due it to being straightforward and logical. While this may be true, it is important to describe the method and standardize it, in order for its straightforward approach to be widely assimilated and for it to become useful in different clinical and surgical situations. The author is unaware of any similar procedure that may have been previously published or detailed in the 57 articles on "biopsies" that have been researched. The same situation applies to the references listed in the present study,1-12 allowing the inference that this is probably an original piece of research.
For this reason, there are no specific bibliographic references in the present article, with the exception of two, 13 and 14, which serve only for compliance reasons.
Although it is difficult to prove the usefulness of oriented biopsies due to the variability of the clinical and surgical circumstances, the author has reviewed the cases in which the method was applied in 173 situations in the previous five years, noting that in 93% of cases the histological information obtained was important in the implementation and completion of various clinical and surgical situations.
The data obtained can be summarized and grouped as described in the section Situations of applicability of the technique.
In cases where the oriented biopsy is considered as an excisional biopsy, the surgeon has to relativize the findings, understanding that in certain situations, if the ellipsis was very narrow and the tumor found to be predominantly infiltrative, the presence of the free margin in the longitudinal direction does not mean that the lateral margin is free. In this case, transverse serial sections along the piece, with free margins do not guarantee that the tumor has been completely removed.1
Due to the fact that in many situations the tumor can hardly be seen, dermoscopy can be a decisive factor indicating the need for surgical intervention.2 However, it is not always sufficiently clarifying. In such cases, confocal microscopy would be considerably useful in spite of its limited ability to offer deep assessments. As this technology is still very expensive and is not yet widely available, the use of dermoscopy combined with oriented biopsies can provide extremely important data to allow better surgical planning.
Performing multiple punch biopsies does not amount to an equivalent procedure, as tumors are not always continuous. An oriented biopsy containing a tumor may reveal sites that do not contain a tumor, whereas a punch biopsy could prove negative. On the other hand, the positivity of the punch does not mean that the tumor can extend far beyond that point.
Recurrent tumors are usually adjacent to an area of scarring. Many surgeons advocate the complete removal of the scar, as it can be frustrating to prove through micrographic surgery whether it was free of a tumor (which could be growing in another direction). In such cases, performing an oriented biopsy in the pre-operative assessment phase, could better guide the micrographic surgery, helping it to fulfill its primary role: to remove only the tumor.
The concept of an oriented biopsy derives closely from surgical excision with microscopic control of the margins, i.e. from the understanding of the logics of the micrographic surgery. The more the subject is known, the more informative the oriented biopsies can be. Also, it is very important to rely on a laboratory that is familiar with these techniques. In the absence of a laboratory able to correctly perform the procedure, a surgeon who has an in-depth understanding of micrographic surgery can provide adequate guidance.
1. Kimyai-Asadi A, Goldberg LH, Jih MH. Accuracy of serial transverse cross-sections in detecting residual basal cell carcinoma at the surgical margins of an elliptical excision specimen. J Am Acad Dermatol. 2005;53(3):469-74.
2. Kopke LF. A dermatoscopia na detecção precoce, controle e planejamento cirúrgico dos carcinomas basocelulares. Surg Cosmet Dermatol. 2011;3(2):103-8.
3. Werner B. Biopsia de pele e seu estudo histológico. Por quê? Para quê? Como? Parte I. An Bras Dermatol. 2009;84(4):391-5.
4. Werner B. Biopsia de pele e seu estudo histológico. Por quê? Para quê? Como? Parte II. An Bras Dermatol. 2009;84(5):507-13.
5. Miller SJ. II. Biopsy techniques for suspected nonmelanoma skin cancers. Dermatol Surg. 2000;26(1):91.
6. Mir M, Chan CS, Khan F, Krishnan B, Orengo I, Rosen T. The rate of melanoma transection with various biopsy techniques and the influence of tumor transection on patient survival. J Am Acad Dermatol. 2013;68(3):452-8.
7. Antonio CR, Tímpano DL, Garcia AC. Biópsia. Rev Bras Med. 2010;67(supl. 9):22-32.
8. Gadelha AR. Biópsias de pele. In: Gadelha AR, Costa IMC, editores. Cirurgia dermatológica em consultório. 2ª ed. São Paulo: Editora Atheneu; 2009. p 209-16.
9. Lee KK, Gorman A, Swanson NA. Biopsy Techniques. In: Rigel DS, Friedman RJ, Dzubow LM, Reintgen DS, Bystryn JC, Marks R, editors. Cancer of the Skin. Philadelphia: Elsevier Saunders; 2005. p. 467-75.
10. Perez MI, Lodha R, Nouri K. Técnicas de biópsia cutânea. In: Nouri K, Leal-Khouri S, editores. Técnicas em cirurgia dermatológica. Rio de Janeiro: DiLivros Editora; 2005. p. 75-9.
11. Sanches SRA, Sanches MD. Biópsias. In: Savassi-Rocha PR, Sanches SRA, Savassi-Rocha AL, editores. Cirurgia de Ambulatório. Rio de Janeiro: Medbook;2013. p. 219-34.
12. Garcia C. Skin Biopsy Techniques. In: Robinson JK, Hanke CW, Sengelmann RD, Siegel DM, editors. Surgery of the Skin - Procedural Dermatology. Philadelphia: Elsevier Mosby;2005. p 203-12.
13. Sampaio SAP, Rivitti EA, editores. Dermatologia. 3a ed. São Paulo: Artes Médicas Ltda; 2007. p. 1474.
14. Olbricht S. Técnicas de biopsia e excisões básicas. In: Bolognia JL, Jorizzo J.L, Rapini R, editors. Dermatologia. 2a ed. Philadelphia: Elsevier Mosby;2008. p. 2209-24.
This study was performed in the author's private practice - Florianópolis (SC), Brazil.
 All content the journal, except where identified, is under a Creative Commons Attribution-NonCommercial 4.0 International license - ISSN-e 1984-8773
All content the journal, except where identified, is under a Creative Commons Attribution-NonCommercial 4.0 International license - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}