


Diego Leonardo Bet1; Érico Pampado Di Santis2; César Augusto Cardoso3; Sérgio Henrique Hirata4; Marcia Lanzoni de Alvarenga5; Samuel Henrique Mandelbaum6
Keywords: DERMOSCOPY; HUTCHINSON'S MELANOTIC FRECKLE; KERATOSIS, ACTINIC; FACE.
Early diagnosis is the cornerstone of managing malignant melanocytic lesions. The authors highlight that this is a crucial role of dermatologists, and that there is a daily challenge in achieving a complete dermatological examination of their patients. Mucous membranes are still neglected,1 and many patients with mucosal melanoma report that they have had undiagnosed pigmented lesions for months or years.2 The authors acknowledge the technical difficulty of carrying out the diagnosis of mucosal lesions, whose clinical signs do not always help in the differential diagnosis from benign pigmented lesions-which constitute the vast majority-and the rare malignant lesions.3 The criteria of classical dermatoscopy of skin lesions are not directly applied to mucosal lesions, however in spite of the few studies in this area, this examination technique may prove very useful for the rational selection of lesions that deserve pathological study.
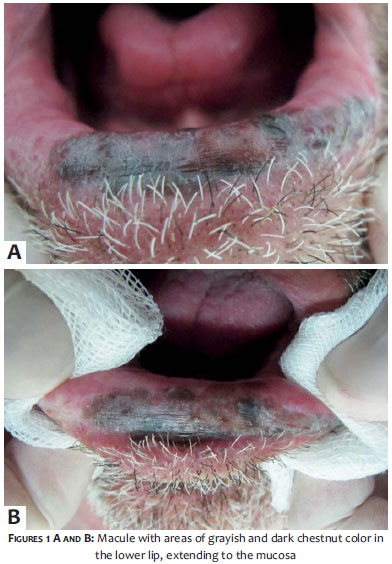
Linked to this paper's subject, the authors present the case of a 64-year-old Caucasian male patient, a former smoker, who reported the appearance and growth of a blackish spot on the lower lip, four years before. Clinical examination revealed that the lesion extended from the center of the lip up to the mucosa, measuring 4 x 1cm (Figure 1).
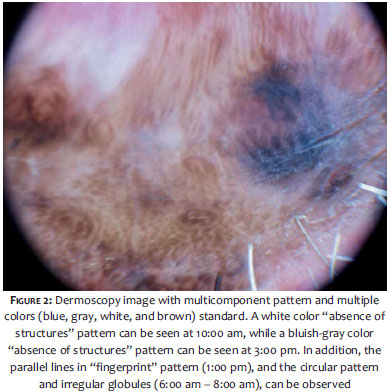
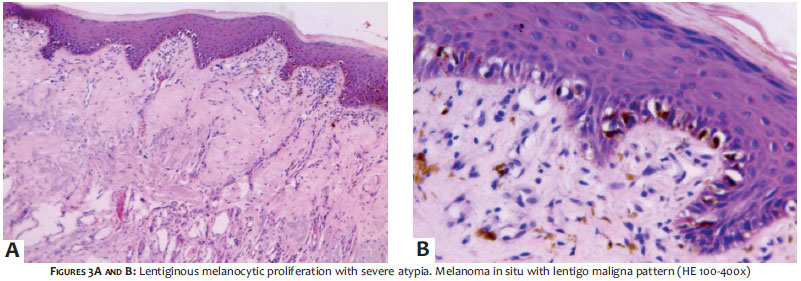
Dermoscopic examination found that the pigmented lesion presented a multicomponent pattern (Figure 2). Excisional biopsy was performed, with histopathology demonstrating melanoma in situ with lentigo maligna pattern (Figure 3). The patient is well and has been monitored for two years after the widening of margins by1cm (Figure 4).
Primary melanomas of the lip are rare, representing 0.05-0.31% of all melanomas and 0.3-2.2% of head and neck melanomas. They predominate in male patients (2:1), and usually occur after the age of 50, with the extensive superficial variant being the most common type. These lesions have aggressive behavior, with reported recurrence of 40%, metastases in 36% and deaths in 60% of patients.4
In 2011, a retrospective multicenter study coordinated by the International Dermoscopy Society3 that included 140 pigmented lesions of mucous membranes, has proposed two simple and very useful models for differentiating benign from malignant lesions.
In the first model, the presence of blue, gray, or white color occurred in100% of the malignant lesions in the study; this fact was considered the main feature in differentiating malignant from benign lesions in the study (100% sensitivity and 64% specificity for melanomas). A pattern of an "absence of structures"-which is defined as the absence of other identifiable patterns (such as dotted, globular, circles, or linear) regardless of color-was also statistically significant. This pattern was present in 100% of melanomas, but also in half of the benign lesions (53.2%). However, in the latter they were usually brown in color, and always featured an absence of blue, gray, and white colors. When added to the color model, the pattern "absence of structures" increases the specificity for melanoma from 64% to 82%, even if present only in some areas of the lesion. Due to its high specificity, it is worth noting the importance of the "multicomponent pattern" (presence of three or more patterns in the same lesion) in other case series reported in the literature. 5
In the present case, it is important to note that the dermoscopy shows a wealth of signals that are not seen with the naked eye. By applying the new diagnostic models, the authors corroborate their validity for they have found not one, but three colors deemed suspect: blue, gray, and white-in addition to brown-as well as the pattern "absence of structures". The authors have also considered that the other three patterns -parallel lines in "fingerprint" pattern, circular pattern and atypical globular pattern- characterize the lesion as having a multicomponent pattern, further reinforcing the suspicion of malignant melanocytic lesion.
It is necessary to consider that despite the great variationin patterns associated with benign mucosal lesions, the identification of the suspected color model with the presence of the pattern "absence of structures" seems to be very useful for a more rational selection of lesions to be excised for anatomical pathological examination.
Last but not least, the authors provide some important guidelines for good dermoscopic examination of the mucous membranes: proper positioning of the patient for examination; using PVC film to protect the dermatoscope from direct contact with the lesion; obtaining digital images of the lesion for analysis on the computer rather than performing analysis on the patient. In the authors' experience, these tips make the procedure easier, safer, and also more acceptable to the patient.
1. Hajar-Serviansky T, Gutierrez-Mendoza D, Galvan IL, Lammoglia-Ordiales L, Mosqueda-Taylor A, Hernandez-Cázares M de L, et al. A case of oral mucosal melanoma. Clinical and dermoscopic correlation. J Dermatol Case Rep. 2012;6(1):1-4.
2. Blum A. Who examines the oral mucosa during the total body skin examination?. Hautarzt Z Für Dermatol Venerol Verwandte Geb. 2012;63(11):899-902.
3. Blum A, Simionescu O, Argenziano G, Braun R, Cabo H, Eichhorn A, et al. Dermoscopy of pigmented lesions of the mucosa and the mucocutaneous junction: results of a multicenter study by the International Dermoscopy Society (IDS). Arch Dermatol. 2011;147(10):1181-7.
4. Matsushita S, Kageshita T, Ishihara T. Comparison of dermoscopic and histopathological findings in a mucous melanoma of the lip. Br J Dermatol. 2005;152(6):1324-6.
5. Lin J, Koga H, Takata M, Saida T. Dermoscopy of pigmented lesions on mucocutaneous junction and mucous membrane. Br J Dermatol. 2009;161(6):1255-61.
This study was performed at the Hospital do Servidor Público Municipal de São Paulo (HSPM/SP) - São Paulo (SP), Brazil and at the Hospital Universitário de Taubaté (HUT) - Taubaté (SP), Brazil.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}