


Guilherme Bueno de Oliveira1; Natália Cristina Pires Rossi2; Carlos Roberto Antônio3; João Roberto Antônio4
Keywords: LIPOID PROTEINOSIS OF URBACH AND WIETHE; AMBULATORY SURGICAL PROCEDURES; SURGICAL PROCEDURES, MINOR; CLINICAL EVOLUTION.
Lipoid proteinosis (LP), also known as cutaneous mucosal hyalinosis, is a rare recessive multisystem autosomal genodermatosis, with a high incidence of consanguinity. It is characterized by the progressive deposition and accumulation of an amorphous eosinophilic hyaline substance, of glycolipoprotein constitution, periodic acid and Schiff reagent (PAS) positive in the skin, with upper aerodigestive tract and visceral involvement1,2 The disease is attributed to mutations resulting in the loss of the extracellular matrix protein's 1 function (ECM1) of 85 kDa, located on the chromosome 1q21. This protein's function is unknown, although it has an important role in the local physiology and homeostasis. 3,4
It affects both genders equally, with onset in childhood, and is characterized by scarring lesions after minor trauma, and hoarseness. The skin lesions consist of yellowish and ivory color papules, which can be grouped into plaques, located especially on the face, neck, and areas of friction. In the latter it may still appear in the form of nodular lesions.1,3,4 The pharyngeal and oral mucosa presents with diffuse infiltration and a yellowish-white color, a stiffened tongue, culminating with dysphonia (and hoarseness since birth), with those symptoms often being the first manifestation of the disease. In more severe cases, the diffuse infiltration of the pharynx and larynx can cause respiratory distress, sometimes requiring tracheotomy. Infiltration of the genital mucosa may occur. 3-5
The systemic-visceral lesions are characterized by orthodontic abnormalities, intracranial calcifications, epilepsy attacks, pigmentary disorders, diabetes mellitus and porphyria. LP has an insidious, chronic, and benign course, not yet having effective treatment.6-10
The objective of the present study is to describe the follow-up of a female patient duringa twenty-five year development, highlighting the importance of dermatologic surgery to improve the quality of life forthose patients.
Twenty-eight-year-old Caucasian female patient, born in the state of São Paulo - Brazil, with a history of parental consanguinity (parents are cousins ).
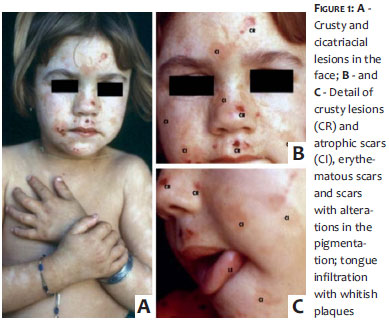
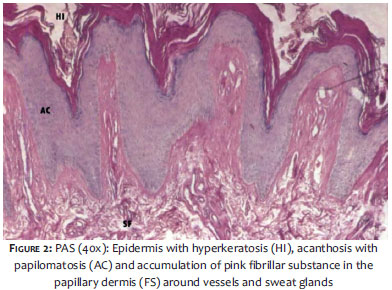
Since the age of two, the patient has had dysphonia and hoarseness associated with skin lesions on the face and limbs, which developed intoblisters, would increased in size and burst, leaving crusts, and erythematous and hypopigmented macules as sequelae. The lesions emerged in outbreaks every six months, with worsening after traumas. At six years of age, there was an appearance of ulcers and nodular lesions on the elbows and forearms. Dermatological examination revealed lesions on the face, some crusty and other hypochromic scarring, and still others depressed hyperchromic, with varicelliform appearance and dimensions ranging from punctate to lenticular. (Figure 1) In the infraorbital region there were small yellowish papules. Elbows and forearms had nodules, exulcerated lesions and areas of thickening bilaterally. Histological examination at six years of age showed an epidermis with hyperkeratosis and papillomatosis, and papillary dermis with accumulation of a pink fibrillar substance around vessels and sweat glands, and atrophy. This substance is PAS positive and diastase resistant. (Figure 2)
Otorhinolaryngologic examination six years of age showed an infiltrated, irregular, and rigid lingual surface with yellowish plaques, (Figure 1) nasal septa with hypertrophied turbinates, thickened pharynx and epiglottis, and vocal cords with normal sensitivity and signs of thickening. Skull MRI showed two images with calcium densities laterally to the cavernous sinus, with symmetrical arrangement and cranial projection. The patient was referred to the neurology service for evaluation and treatment of epileptic seizures.
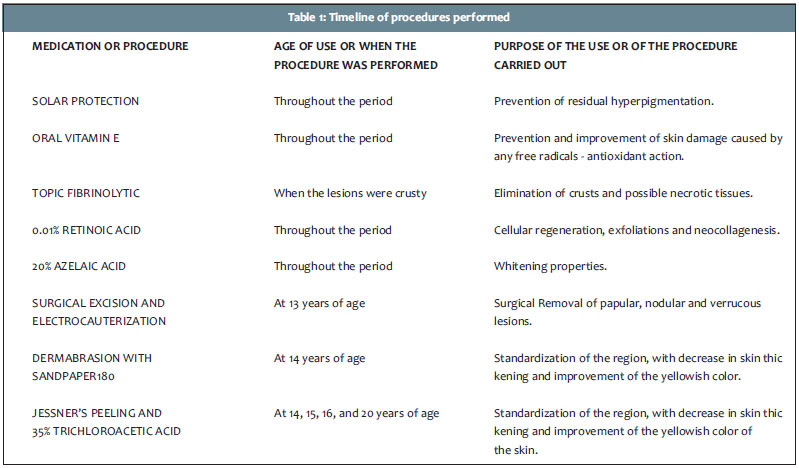
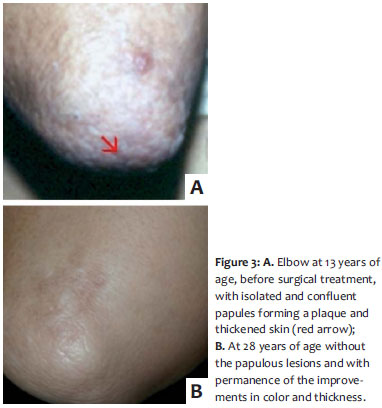
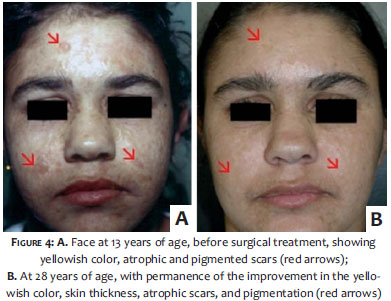
Skin lesions were approached with clinical treatment and surgical procedures. (Table 1) Clinically, there was the introduction of sunscreens with chemical filters and SPFs between 30 and 50, oral vitamin E, fibrinolytic topical cream up to three times daily in the presence of crusty lesions, 0.01% retinoic acid cream at night and 20% azelaic acid cream in the morning before applying sunscreen. Surgically, electrocautery and surgical excision of nodular and verrucous lesions were carried out in the lower and upper eyelids, and elbows (Figure 3); dermabrasion with sandpaper number 180 preceded by local anesthesia with 2% lidocaine was performed in the frontal region, medium chemical peel with Jessner solution and 35% trichloroacetic acid was applied on the whole face, with improvement in the skin-thickening and the yellowish color of the skin. (Figure 4)
Currently, at 28 years of age, only shallow scarring lesions can be seen, with a subtle continuation of the varicelliform aspect, interspersed with skin of normal color in the mid-facial and frontal regions. In the infraorbital region there was an almost complete disappearance of the small yellowish papules. (Figure 5) Three years before, the patient developed diffuse non-scarring alopecia, dysphagia, and dyspaurenia, with the dermatological appearance remaining stable and no new occurrence of lesions. The patient, however, presents resistance to the treatment of seizures and a persistence of dysphonia, hoarseness, and infiltration and hardening of the lingual surface.
LP is an extremely rare, recessive autosomal disease, commonly associated with consanguinity, with approximately 300 cases described in the literature, with the highest prevalence in Sweden and South Africa. 10 In the case ofthe present study, the authors observed the patient's cutaneous appearance with infiltrated skin of yellowish color, similar to the color of ivory, in the face, neck, hands, knees, and elbows. Skin lesions manifested in various developmental stages: papulous, nodular, keratotic, and verrucous, leading to the formation of varicelliform scars. These have as worsening factors, mechanical trauma and exposure to the sun. The alterations in the skin of the eyelids is called "Moniliform Blepharosis". 10 The mucosal condition was characterized by dysphonia and hoarseness from birth, yellow-white infiltrated plaques on the lips, tongue, pharynx, and tongue, and a stiffened tongue with impaired mobility. Systemic manifestations that may be present and have been observed in patients were alopecia, hypohidrosis, nail and tooth abnormalities, intracranial calcifications, and epilepsy, the last two treated by a Neurologist. 1,5
LP usually has a chronic and benign course, requiring ambulatory monitoring and support for life, for there is no known effective treatment.2,10 Clinical therapeutic options include: oral retinoids or D-penicillamine 8-10 and surgical therapy consisting of dermabrasion, chemical exfoliation, or 10,600nm CO2 laser.6,7 The use of surgical dermabrasion with sandpaper number 180 and chemical exfoliations with Jessner's solution and 35% trichloroacetic acid, showed similar results to those in the researched literature. The use of a topical retinoid during the entire period enables cell regeneration, constant exfoliation, and synthesis of new collagen, bringing benefits to the final cosmetic result.
In the present case report, the clinical and surgical treatments used in the patient during the 25-year follow-up showed satisfactory results for the control of dermatological signs such as scar lesions on the face, infraorbital region, and upper and lower eyelids, with significant improvement in the appearance and, more markedly, of her quality of life. As the lesions are not prone to natural involution, the choice for surgical therapy is mandatory to eliminate papular, nodular, and vegetating lesions, as well as the use of dermabrasion and chemical exfoliations for the improvement of the skin thickening and yellowish color.
The present study is aimed at highlighting that, even with the absence of a definitive and effective treatment described in the researched literature, clinical and surgical procedures should be encouraged in the management of patients bearing LP. Given that the clinical profile has an onset in childhood or early adolescence, procedures should be performed progressively, with the use of the available therapeutic armamentarium according to the appropriate indications, aiming at improving the dermatological signs. 6-10 In this manner, it is possible to prevent the origin of certain stigmas that affect the quality of life of patients.
1. Santana N, Devi BK, Ramadoss T, Sumati T, Prasad S, Swamy S. Lipoid proteinosis: a case report. Quintessence Int. 2010;41(3):e51-3.
2. Yadava U, Khurana N, Mehta S. Lipoid proteinosis: a case report. Pathology. 2006;38(6):600-2.
3. Horev L, Wollina DU, Potikha T, Hafner A, Ingber A, Liu L, et al. Lipoid proteinosis: identification of two novel mutations in the human ECM-1 gene and lack of genotype-phenotype correlation. Acta Derm Venereol. 2009;89(5):528-9.
4. Fujimoto N, Terlizzi J, Aho S, Brittingham R, Fertala A, Oyama N, et al. Extracellular matrix protein 1 inhibits the activity of matrix metalloproteinase 9 through high-affinity protein/protein interactions. Exp Dermatol. 2006;15(4):300-7.
5. Kroukamp G, Lehmann K. Treatment of laryngeal lipoid proteinosis using CO2 laser. S Afr Med J. 2007;97(2):90,92.
6. Bannerot H, Aubin F, Tropet Y, Najean D, Blanc D. Lipoid proteinosis: importance of dermabrasion. Apropos of a case. Ann Chir Plast Esthet. 1998;43(1):78-81.
7. Toosi S, Ehsani AH. Treatment of lipoid proteinosis with acitretin: a case report. J Eur Acad Dermatol Venereol. 2009;23(4):482-3.
8. Gruber F, Manestar D, Stasic A, Grgurevic Z. Treatment of lipoid proteinosis with etretinate. Acta Derm Venereol. 1996;76(2):154-5.
9. Kaya TI, Kokturk A, Tursen U, Ikizoglu G, Polat A. D-penicillamine treatment for lipoid proteinosis. Pediatr Dermatol. 2002;19(4):359-62.
10. Lima LR, Mulinari-Brenner FA, Manfrinato LC. Lipoidoproteinose - relato de dois casos. An Bras Dermatol. 2003;78(6):723-7.
This study was performed at the Faculdade de Medicina Estadual de São José do Rio Preto (FAMERP) - São Paulo (SP), Brazil.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}