


Sadamitsu Nakandakari1; Gabriela Franco Marques2; Cleverson Teixeira Soares3; Lívia Soares Santino Santos4; Juliana Martins Prazeres Sousa5
Keywords: NAILS; NAILS, MALFORMED; NEOPLASMS.
Onychomatricoma (OM) is a rare benign tumor that originates from the nail matrix and the underlying stroma.1,2 It was first described by Baran and Kint in 1992.3 Since its first description a few more than 40 cases have been reported in the international literature.4
OM affects middle-aged men and women evenly and is more prevalent in Caucasians.4-6 It is the only nail tumor in which the alteration of the nail plate is actively produced by the lesion.6 Although its etiology is not yet understood, history of trauma is referred as a predisposing factor.1,4
The picture is usually asymptomatic, however there are four key clinical features for the diagnosis: presence of a yellowish longitudinal stripe of variable thickness; splinter hemorrhages involving the proximal portion of the nail plate; longitudinal grooves associated with the transverse hypercurvature; and fingerlike projections emerging from the matrix-the latter being responsible for the production of small cavitations observed from the free border of the nail plate. 1, 2, 4, 6
The present study reports three OM cases, emphasizing the main clinical aspects, dermoscopic findings, and surgical treatment.
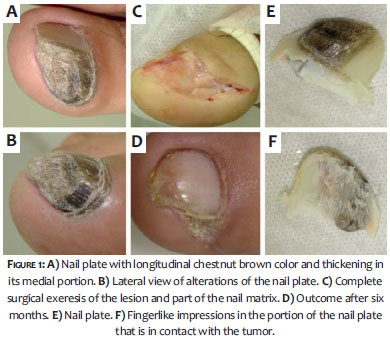
Case 1: A fifty-three-year-old Caucasian man referred for thickening of the nail of the right hallux for the preceding five years. On examination, the nail plate was perceived to be thickened and of chestnut brown color in its medial portion (Figures 1A and B). The nail plate was removed, and a chestnut grayish homogeneous mass could be observed in the matrix region. The lesion was surgically excised (Figure 1C), and the histology revealed features of OM. There was no recurrence six months after the surgery. (Figure 1D)
The nail plate had a hard consistency and presented cavitations in its proximal portion. (Figures 1E and F)
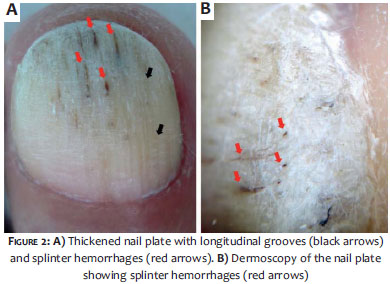
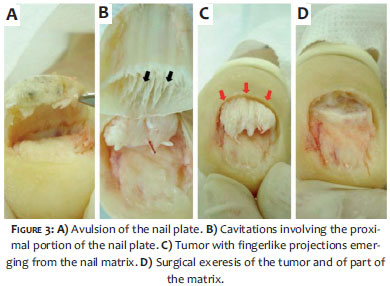
Case 2: A forty-two-year-old Caucasian woman presented with a thickening of the nail of the left hallux for ten years, with an absence of associated symptoms. Upon examination it presented with a thickened and yellowish nail with splinter hemorrhages (Figure 2). Surgery with avulsion of the nail plate was carried out (Figure 3A). The nail plate had cavitations in its proximal portion (Figure 3B) and had coupled with the tumor through fingerlike projections in the matrix (Figure 3C), which was excised (Figure 3D). Anatomical pathology confirmed the OM diagnosis. There was no recurrence after six months, and nail growth took place without sequelae.
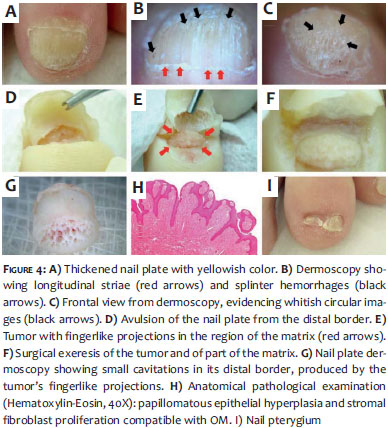
Case 3: A fifty-five year-old Caucasian woman complained of asymptomatic thickening of the nail plate of the left third toe for two years. Upon examination, thickened, yellowish nails were observed, with longitudinal grooves and transverse hypercurvature (Figure 4A). Dermoscopy evidenced whitish striae and splinter hemorrhages (Figure 4B); whitish circular images (Figure 4C) were identified in the frontal view.
Avulsion of the nail plate was carried out (Figure 4D) and after its elevation a tumor with fingerlike projections in the area of the matrix was observed (Figure 4E). The complete excision of the lesion (Figure 4F) was performed. Dermoscopy of the nail plate showed small cavitations involving the proximal portion (Figure 4G). Histopathology was compatible with OM (Figure 4H). Six months after treatment there was no recurrence of the tumor, however the patient developed nail pterygium (Figure 4I).
OM is usually asymptomatic and most patients only seek medical care many years after its emergence.4,6
In the reported cases, the patients had no associated symptoms, and the main complaint was the thickening of the nail plate. That fact can be explained by the slow growth inherent to the tumor. Studies on markers cannot distinguish whether the OM is a tumor or a reactive lesion, although it has been suggested that it can be a hamartoma of epithelial and connective tissue mimicking matrix structures.3 Trauma history was not mentioned in any of the cases, and as described in the literature, the etiology remains obscure. 3, 5, 6
The tumor is more common in middle-aged Caucasians,5-8 as in the cases reported. Although descriptions of involvement of the fingers are more common than those involving toes,8 all reported cases had involvement of toenails-two of them in the hallux and one in the third toe.
The four main clinical features in the diagnosis might have variable expression in cases where the color alteration of the nail is more exuberant-such as in Case 1-and others where the diffuse thickening of the nail and the presence of splinter hemorrhages are more evident-such as in Cases 2 and 3. The fourth typical characteristic of the tumor, which corresponds to finger-like projections emerging from the matrix, can only be examined during surgery. 3, 6
Dermoscopy assists in the visualization of splinter hemorrhages in the proximal portion of the nail plate and longitudinal whitish grooves, the latter corresponding to the channels of the nail plate. 2, 6 A frontal view of the nail plate can also show circular whitish areas, some with bleeding fragmentsembedded within, as shown in Case 3.
The bioposy of the lesion is crucial for a definitive diagnosis, which is histological. OM is a fibroepithelial tumor composed of two distinct parts. The proximal zone is characterized by deep epithelial invaginations and fibrillary and fibrotic stroma; the distal zone has multiple digitations along its axis. Immunohistochemistry is of great diagnostic aid. The AE1/AE3 antibody is a potential marker for OM. There is also a diffuse expression of CD34, whereas CD99 markers, S-100 protein, epithelial membrane antigen, actin, and desmin are negative.5, 7, 8
Among the complementary tests, ultrasound is useful for observing the tumor in the matrix area, beneath the proximal nail fold. If performed in the nail plate region, it is not instructive due to the thickening of the nail plateforming an acoustic shadow, which hampers the identification of the tumor. On the other hand, MRI can yield information both relative to the matrix and the nail plate.4 Another recently described diagnostic method suggests the clipping of the distal part of the nail and anatomical pathological examination.9 Nevertheless, in most cases the clinical and dermoscopic examinations, associated with anatomical pathological examination, are sufficient for diagnostic clarification, as in the cases reported in the present study in which no complementary examinations were required.
The differential diagnosis should be carried out with squamous cell carcinoma, verruca vulgaris, keratoacanthoma, fibrokeratoma, Bowen's disease, fungal, and bacterial infections. There are also atypical cases described as a verrucous surface tumor located in the lateral nail fold, total onychodystrophy and a variation of the pseudo-fibrokeratoma type. 2, 4, 5
In the face of a suspected diagnosis, patients should undergo avulsion of the nail plate for matrix analysis. 3, 10 It is worth noting that in the three cases described, the nail plate hada hard consistency, making handling difficult during surgery. In all cases tumors with fingerlike projections in the matrix could be observed, which were responsible for the formation of small cavitations observed in the free border of the nail plate. 1, 3, 4
The long-term prognosis is favorable, and growth of the nail can occur later without defects. Some patients, however, develop onychodystrophy.10 Six months after the surgery, patients were reassessed with no evidence of tumor recurrence. Nevertheless, only in Case 2 did the growth of the nail plate occur without sequelae.
The authors can conclude that, despite the rarity of this condition, early diagnosis is key for optimal treatment. It is important to note that the clinical presentation might not present all the typical characteristics of the tumor, and there may be variations among the cases.The authors call attention to the circular whitish areas that contain splinter hemorrhages -visualized during dermoscopy and observed in one of the cases reported-as well as to the hard consistency of the nail plate found during surgery in all cases described.
1. Durrant MN, Palla BA, Binder SW. Onychomatricoma: a case report with literature review. Foot Ankle Spec. 2012;5(1):41-4.
2. Fernández-Sánchez M, Saeb-Lima M, Charli-Joseph Y, Méndez-Flores S, Sánchez-Hernández C, Carbajosa-Martinez J. Onychomatricoma: an infrequent nail tumor. Indian J Dermatol Venereol Leprol. 2012;78(3):382-3.
3. Baran R, Kint A. Onychomatrixoma: filamentous tufted tumor in the matrix of a funnel-shaped nail: a new entity (report of three cases). Br J Dermatol 1992;126(5):510-5.
4. Baran R, Nakamura R. Doença das Unhas: do diagnóstico ao tratamento. Rio de Janeiro: Elsevier; 2011.
5. Perrin C, Goettmann S, Baran R. Onychomatricoma: clinical and histopathologic findings in 12 cases. J Am Acad Dermatol 1998;39:560.
6. Di Chiacchio N, Tavares GT, Padoveze EH, Bet DL, Di Chiacchio NG. Onicomatricoma. Surg Cosmet Dermatol. 2013;5(1):10-4.
7. Cañueto J, Santos-Briz A, García JL, Robledo C, Unamuno P. Onychomatricoma: Genome-wide analyses of a rare nail matrix tumor. J Am Acad Dermatol. 2011;64(3):573-8.
8. Perrin C, Baran R, Balaguer T, Chignon-Sicard B, Cannata GE, Petrella T, Michiels JF. Onychomatricoma: new clinical and histological features. A review of 19 tumors. Am J Dermatopathol. 2010;32(1):1-8.
9. Tosti A, Romanelli P, Zaiac M, de Farias DC, Miteva M. Nail Clipping Diagnosis of Onychomatricoma. Arch Dermatol. 2011;147(9):117-8.
10. Becerro de Bengoa R, Gates JR, Losa Iglesias ME, Alija Martinez B. Rare toenail onychomatricoma: surgical resolution of five cases. Dermatol Surg. 2011;37(5):709-11.
This study was performed at Instituto Lauro de Souza Lima (ILSL) - Bauru (SP), Brazil.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}