


Elen Violeta Sousa Santos Cela1; Márcia de Britto da Rocha1; Chang Yung Chia2; Camille Furtado Alves3
Keywords: BURNS; HAIR REMOVAL; GLUCOCORTICOIDS; WETTING AGENTS.
Burns are one of the most common household and workplace accidents in modern society. First-degree and superficial second-degree burns are self-limited and heal without leaving scars. However, intense pain and medium- to long-term sequelae may remain as a function of the type and frequency of the burns, e.g., ionizing radiation.1,2 First-degree burns are not considered a serious problem, and until recently, there was no "ideal" or efficacious treatment for the pain and inflammatory reactions caused by various types of first-degree burns, e.g., scalding, exposure to sunlight, ionizing radiation, etc.3
An emulsion based on crabwood oil (COE), also known by its commercial brand Tegum,® has been used in the prevention and treatment of radiation dermatitis, post-chemotherapy skin sequelae, decubitus ulcers, and post photo-epilation burns. In a previous pilot study conducted by the present authors on nine patients, intense pulsed light (IPL) photoepilation was an optimal experimental model to investigate the treatment of first-degree burns because the burns that occurred as side effects were controlled based on the patient's phototype.4 Therefore, the therapeutic effect of COE used on one side of the patient could be compared to the effects of the low-potency corticoid desonide applied on the other side of the patient. A comparison was thus performed at the individual level using a double-blind model, in which the patients were asked to assess the progression of pain in the treatments, and the medical observer assessed the changes in erythema. The previous pilot study concluded that COE was efficacious, safe, and comparable to desonide in regards to pain relief and the reduction of inflammation associated with first-degree burns.4 The aim of the present study was to confirm the previous results using 33 patients and statistical analyses. We also aimed to establish whether a seven-day COE treatment prior to epilation is beneficial according to the protocol for the prevention and treatment of radiation dermatitis.
The present prospective, comparative, double-blind study was conducted on 33 patients. The inclusion criteria were female gender, 18 to 45 years old, phototypes I to III on the Fitzpatrick scale, and healthy skin at the axillae. The exclusion criteria were active dermatosis; skin spots at the axillae; pregnancy or breastfeeding; allergies to the tested agents; intense exposure to the sun 15 days prior to the experiment; a history of illness aggravated or triggered by ultraviolet radiation; the use of immunosuppressants, anti-histamines, non-hormonal anti-inflammatory agents, or systemic corticoids up to two weeks before the experimental procedure; the use of oral or topical vitamin A acid and/or derivatives up to one month before the experimental procedure; cosmetic or dermatological treatment involving the axillae one month before the study; immunodeficiency; a history of atopy; dermographism; previous or ongoing participation in other clinical studies that ended fewer than seven days before recruitment; or professionals involved or interested in the study. The aims and procedures of the study were explained to the participants who fulfilled the inclusion and exclusion criteria. The participants were then asked to sign an informed consent form. The study was conducted in compliance with the norms recommended by the 2000 Declaration of Helsinki.
The participants were assessed and requested to prepare for the experimental procedure in the following manner: beginning seven days prior, the participants used COE on one axilla three times per day and a hydrating cream on the opposite axilla, which had a color, odor, and consistency identical to COE. The hydrating cream and the COE were delivered in identical containers randomly labeled "right" or "left". No product, local or systemic analgesics, or anti-inflammatory agents were used on the day of the procedure. The participants' axillae were epilated by a dermatologist using the standard IPL method with the parameters adjusted to the patients' phototype and the device instructions. The participants assessed pain by comparing both axillae on a visual analogue scale (VAS) ranging from 0 (zero), no pain, to 10, maximum pain (Figure 1). Subsequently, a second dermatologist assessed inflammation as a function of the degree of erythema according to a modified color scale ranging from 0 (zero), no erythema, to 10, maximum erythema (Figure 2). Both the patient and the assessing dermatologist were blind to the product applied to the axillae during the preparation stage or procedure.
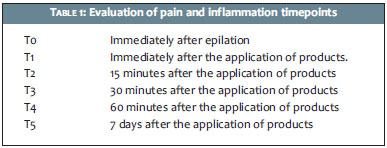
Pain and inflammation were assessed at the following time points: T0-immediately after epilation; T1-immediately after application of the test products on the axillae; T2-15 minutes after application of the test products; T3-30 minutes after application of the test products; T4-60 minutes after application of the test products; and T5-seven days after the procedure (Table 1).
Statistical methods
A Wilcoxon signed-rank test was used in an inferential analysis to establish whether there was significant variation in the pain and erythema scores and in the absolute and relative deltas of the scores following treatment with desonide and COE. Non-parametric tests were used because the scores did not exhibit a Gaussian distribution, as a function of the discrete nature of the data, and the assumption of normality was rejected by a Kolmogorov-Smirnov test. The significance level was established as 5%. The statistical analyses were performed using the SAS 6.11 software (SAS Institute, Inc., Cary, NC).
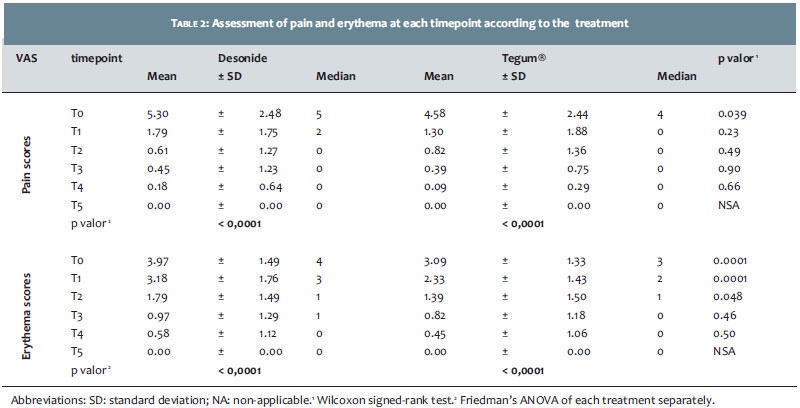
The significant variation in the pain and erythema scores following treatment with desonide and COE was investigated. Table 2 describes the means, standard deviations (SD), and medians of the pain and erythema scores at each time point per treatment (desonide and COE) and the descriptive level of the Wilcoxon signed-rank test (p value). A Friedman's ANOVA was performed separately for each treatment to establish whether there was a significant decrease in the scores at the five time points.
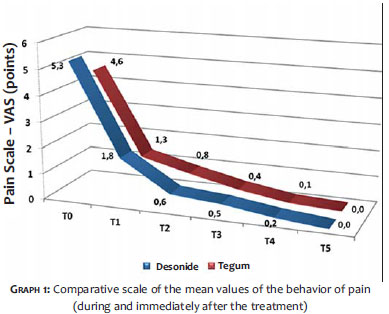
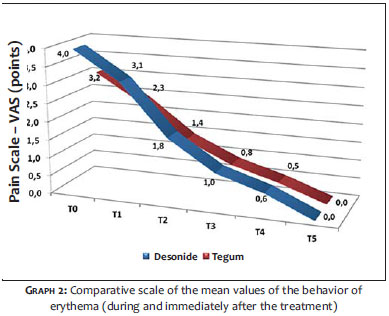
The pain (p < 0.0001) and erythema (p < 0.0001) scores significantly decreased in both treatments, which emphasizes the efficacy of both medications. Treatment with COE was associated with significantly lower pain scores at T0 (p = 0.039) and significantly lower erythema scores at T0 (p = 0.0001), T1 (p = 0.0001), and T2 (p = 0.048) compared to desonide (Graphs 1 and 2).
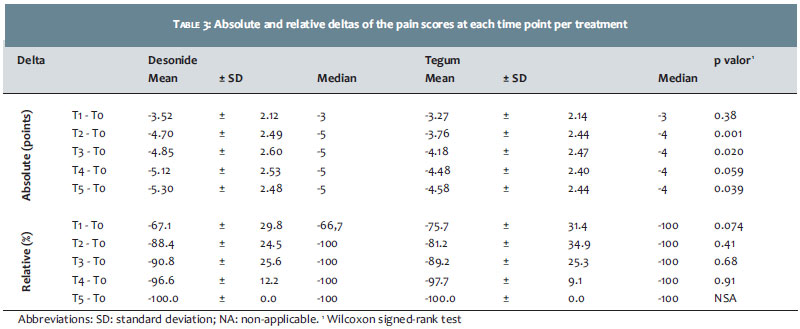
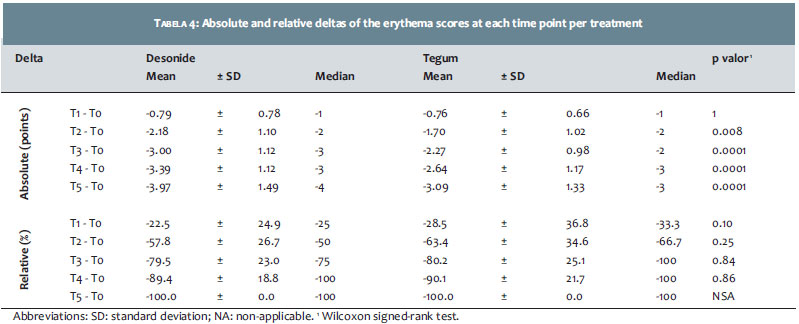
Additionally, the significant variation in the absolute and relative deltas of the pain and erythema scores was investigated for both treatments. Tables 3 and 4 describe the means, SD, and medians of the absolute (scores) and relative (percentage) deltas at each time point per treatment (desonide and COE) and the corresponding descriptive level of the Wilcoxon signed-rank tests (p value). Absolute delta corresponds to the variation between two time points, e.g., T1 to T0, expressed as scores. Negative absolute delta indicates the score reduction from T0 to T1. Relative delta corresponds to the percentage of variation between T1 and T0, (T1-T0) / T0 x 100. Negative relative delta indicates the percentage of reduction relative to T0.
In addition, the relative variation was investigated because a significant difference was observed in the pain and erythema scores between the treatments at T0, i.e., the treatments differed at the baseline.
Treatment with COE was associated with an absolute reduction in pain scale scores, which were significantly lower compared to the desonide treatment at T2 (p = 0.001), T3 (p = 0.020), and T5 (p = 0.039) relative to T0. No significant relative reduction (%) was observed at any time point between the treatments.
Treatment with COE was associated with an absolute reduction in the erythema scale scores, which were significantly lower compared to the desonide scores at T2 (p = 0.008), T3 (p = 0.0001), T4 (p = 0.0001), and T5 (p = 0.0001) relative to T0. No significant relative reduction (%) was observed at any time point between the treatments.
The pain and erythema baseline scores for the COE treatment were significantly lower (approximately one point) compared to desonide; however, COE exhibited a significantly smaller decrease compared to desonide (approximately one point), thus indicating a "compensation". Therefore, COE induced a similar percentage of reduction compared to desonide and achieved similar levels on the VAS beginning at T1 for pain and T3 for erythema. There was a significant difference when the descriptive level (p value) ranged from 0.05 to 0.10.
The equivalent efficacy of COE and desonide regarding pain relief and the improvement of erythema in first-degree burns was confirmed. The axilla previously prepared with COE exhibited less pain and erythema immediately after the induction of burns compared to the axilla prepared using the placebo and treated with desonide. These results might indicate that COE has a protective effect when it is used seven days prior to a radiotherapy procedure according to the protocol for skin preparation in patients with breast cancer.
First-degree burns are described as limited to the epidermis; however, injury might not be apparent and might extend into deeper layers and generate permanent sequelae. Following thermal aggression, the burned area exhibits a central area of necrosis and a peripheral area of stasis surrounded by hyperemia.5 For sunburns, ultraviolet radiation causes irreversible damage to the cell DNA, leading to early aging and neoplasms over time.6 In the acute phase, an inflammatory reaction occurs with the release of cytokines and free radicals and the activation of mast cells, which perpetuate pain and hyperalgesia.7 Laser burns are classified as photothermal, photomechanical, and photochemical; of these, the thermal variety is the most significant.8 Radiation causes free radical production, which results in oxidative stress and damage to cell DNA.1,2
Rupture of the protective barrier and homeostasis of the corneal layer is common to all varieties of superficial burns, as is the production of free radicals and inflammation, which make pain more intense and may perpetuate tissue injury. An ideal treatment involves topical replacement of the intracellular lipids (cholesterol, free fatty acids, and ceramide) that compose the corneal barrier to induce quick replacement and control fluid loss and exert anti-inflammatory and anti-oxidative effects to reduce tissue damage and pain.8 Several agents were tested as treatments for superficial burns. In a review performed by Han and Maibach (2004) on the prevention and treatment of sunburns, topical d-alpha tocopherol reduced swelling, erythema, and skin sensitivity induced by ultraviolet radiation in hairless mice. The authors' review concluded that there are no clinical studies showing that corticosteroids, non-steroidal anti-inflammatory, anti-histamine, or anti-oxidant agents effectively treat acute sunburns and that the most reasonable treatment is to induce symptom relief using emollients and pain control medication.6 Vaseline® petroleum jelly occludes and blocks skin perspiration; however, Xu and Xiao (2003) observed that it might "suffocate" and macerate the tissue.9 In a study on burn-wound healing in mice that compared three treatments and a control without a treatment, the Vaseline® -treated group exhibited fewer contractions compared to the controls.10 Corticosteroids are the most powerful anti-inflammatory agents, but their atrophic action extends across the epidermis and dermis and causes a nearly immediate reduction of extracellular production, mainly of hyaluronans.11,12 The immediate cooling of burns might relieve pain but does not prevent secondary hyperalgesia.7
Depending on its composition, an emulsion might contribute more than symptom relief and hydration to treating first-degree burns and might also exert therapeutic effects for conditions with disruptions of the epidermal barrier or inflammation. The topical replacement of three types of intracellular lipids in the corneal layer (free fatty acids, cholesterol, and ceramide) accelerates the regeneration of the epidermal barrier.8 Lipid mixtures were efficient in allergic, contact, and atopic dermatitis.13-14 Fatty acids increase innate immunity.15 Oleic acid accelerates wound healing, regenerates the epidermal barrier, has bactericidal effects against methicillin-resistant Staphylococcus aureus (MRSA), and exerts anti-inflammatory actions.16-18 In one study, oleic acid increased skin flap survival in rats.19 Melaleuca alternifólia oil is an anti-inflammatory agent with powerful antibiotic action against bacteria (including MRSA), fungi, and viruses.20-22 Crabwood (Carapa guianensis) oil accelerates wound healing in excision, incision, and dead space; exhibits powerful anti-inflammatory and anti-allergic actions; and might prevent histamine-induced hyperalgesia.23-25 Vitamin A stimulates fibroblast proliferation and collagen production, is an antioxidant, provides protection against ultraviolent radiation, and has anticarcinogenic effects.26-28 Tocopherol protects against DNA damage induced by ultraviolet radiation, reduces the inflammatory response, and is a powerful antioxidant.28-30
Epidermal integrity and homeostasis play an important role in skin wound healing and regeneration. Some evidence indicates that keratinocytes modulate the behavior of the dermal cells in the communication between the dermis and epidermis.31 An emulsion containing a combination of such elements might quickly re-establish epidermal homeostasis, thus reducing inflammation and oxidative stress and, consequently, injury and pain.
Overall, the efficacy of COE was equivalent to that of desonide for pain relief and erythema improvement following superficial burns induced by IPL epilation, thus confirming the results of the pilot study. The axilla subjected to previous preparation with COE for seven days exhibited less erythema and pain immediately after burn induction. These findings might indicate the protective effect of COE on the skin. The preparation regimen used in the present study is also applied in radio and chemotherapy protocols for patients with cancer, and its relevance was confirmed by the present study.
1. Mackanos MA, Helms M, Kalish F, Contaq CH. Image-guided genomic analysis tissue response laser-induced thermal stress. J Biomed Opt. 2011;16(5):058001.
2. Museux N, Perez L, Autrique L, Agay D. Skin burns after laser exposure: histological analysis and predictive simulation. Burns. 2012;38(5):658-67.
3. Proksch E, Jensen JM, Crichton-Smith A, Fowler A, Clitherow J. Rational treatment of patients with first-degree burns. Hautarzt. 2007;58(7):604-10.
4. Cela EVSS, Rocha MB, Gomes TM, Chia CY, Alves CF. Avaliação clínica da eficácia do óleo de andiroba na queimadura pós-depilação com luz intensa pulsada: estudo prospectivo, comparativo e duplo-cego. Surg Cosmet Dermatol. 2012;4(3):248-51.
5. Serra MCVF, Bravo BSF, Castro MCR. Alterações por dano térmico - calor. In: Ramos e Silva M, Castro MCR. Fundamentos de dermatologia. Rio de Janeiro: Atheneu;2009. P. 555-79.
6. Han A, Maibach HI. Management of acute sunburn. Am J Clin Dermatol 2004;5(1):39-47.
7. Werner UM, Lassen B, Pedersen JL, Kehlet H. Local cooling does not prevent hyperalgesia following burn injury in humans. Pain 2002;98(3):297-303.
8. Proksch E, Jensen JM. Skin as an organ of protection. In: Wolff K, Goldsmith LA, Katz SI, Gilchrest BA, Paller AS, Leffell DJ, editors. Fitzpatrick's Dermatology in General Medicine. New York: McGraw Hill; 2012. p. 486-98.
9. Xu RX, Xiao M. The mechanism of burn regenerative therapy and wound healing. The Chinese Journal of Burns Wounds and Surface Ulcers. 2003;4:262-71.
10. Djerrou Z, Maameri Z, Hamdi-Pacha Y, Serakta M, Riachi F, Djaalab H, et al. Effect of virgin fatty oil of Pistacia lentiscus on experimental burn wound's healing in rabbits. Afr J Tradit Complement Altern Med. 2010;7(3):258-63.
11. Schoepe S, Schäcke H, May E, Asadullah K. Glucocorticoid therapy-induced skin atrophy. Exp Dermatol. 2006;15(6):406-20.
12. Gebhardt C, Averbeck M, Diedenhofen N, Willenberg A, Anderegg U, Sleeman JP, N et al. Dermal hyaluronan is rapidly reduced by topical treatment with glucocorticoids. J Invest Dermatol. 2010;130(1):141-9.
13. Bereardesca E, Barbarechi M, Veraldi S, Pimpinelli N. Evaluation of efficacy of a skin lipid mixture in patients with irritant contact dermatitis, allergic contact dermatitis or atopic dermatitis: a multicenter study. Contact Dermatitis 2001;45(5):280-5.
14. Butnariu M, Giuch CV. The use of some nanoemulsions based on aqueous própolis and lycopene extract in the skin's protective mechanisms against UVA radiation. J Nanobiotechnology. 2011;9:3.
15. Nakatsuji T, Kao MC, Zhang L, Zouboulis CC, Gallo RL, Huang CM. Sebum free fatty acids enhance the innate immune defense of human sebocytes by upregulating beta-defensin-2 expression. J Invest Dermatol. 2010;130(4):985-94.
16. Cardoso CR, Souza MA, Ferro EA, Favoreto S Jr, Pena JD. Influence of topical administration of n-3 and n-6 essential and n-9 nonessential fatty acids on the healing of cutaneous wounds. Wound Repair Regen. 2004;12(2):235-43.
17. Chen CH, Wang Y, Nakatsuji T, Liu YT, Zouboulis C, Gallo R, et al. An innate bactericidal oleic acid effective against skin infection of methicillinresistant Staphylococcus aureus: a therapy concordant with evolutionary medicine. J Microbiol Biotechnol 2011;21(4):391-99.
18. Huang CM, Chen CH, Pornpattananangkul D, Zhang L, Chan M, Hsieh MF, et al. Eradication of drug resistant Staphylococcus aureus by liposomal oleic acids. Biomaterials. 2011;32(1):214-21.
19. Hsu OK, Gabr E, Steward E, Chen H, Kobayashi MR, Calvert JW, et al. Pharmacologic enhancement of rat skin flap survival with topical oleic acid. Plast Reconstr Surg. 2003;113(7):2048-54.
20. Brady A, Loughlin R, Gilpin D, Kearney P, Tunney M. In vitro activity of tea-tree oil against clinical skin isolates of methicillin-resistant and - sensitive Staphylococci growing planktonically and as biofilms. J Med Microbiol. 2006;55(Part 10):1375-80.
21. Carson CF, Hammer KA, Riley TV. Melaleuca alternifólia (Tea Tree) oil: a review of antimicrobial and other medicinal properties. Clin Microbiol Rev. 2006;19(1):50-62.
22. van de Sande WW, Fahal AH, Riley TV, Verbrugh H, van Belkum A. In vitro susceptibility of Madurella mycetomatis, prime agent of Madura foot, to tea tree oil and artemisinin. J Antimicrob Chemother. 2007;59(3):553-5.
23. Penido C, Conte FP, Chagas MS, Rodrigues CA, Pereira JF, Henriques MG. Antiinflammatory effects of natural tetranortriterpenoids isolated from Carapas guianensis Aublet on zymosan-induced arthritis in mice. Inflamm Res. 2006;55(11):457-64.
24. Penido C, Costa KA, Pennaforte RJ, Costa MF, Pereira JF, Siani AC, et al. Anti-allergic effects of natural tetranortriterpenoids isolated from Carapas guianensis Aublet on allergen-induced vascular permeability and hiperalgesia. Inflamm Res. 2005;54(7):295-303.
25. Nayak BS, Kanhai J, Milne DM, Pinto Pereira L, Swanston WH. Experimental evaluation of ethanolic extract of Carapa guianenesis L. Leaf for its wound healing activity using three wound models. Evid Based Complement Alternat Med. 2011;2011:419612.
26. Hansen LA, Sigman CC, Andreola F, Ross SA, Kelloff GJ, De Luca LM. Retinoids in chemoprevention and differentiation therapy. Carcinogenesis. 2000;21(7):1271-9.
27. Antille C, Tran C, Sorg O, Carraux P, Didierjean L, Saurat JH. Vitamin A exerts a photoprotective action in skin by absorbing ultraviolet B radiation. J Invest Dermatol. 2003;121(5):1163-7.
28. Maia Campos PM, Gianeti MD, Kanashiro A, Lucisano-Valim YM, Gaspar LR. In vitro antioxidant and in vivo photoprotective effects of an association of bioflavonoids with liposoluble vitamins. Photochem Photobiol. 2006;82(3):683-88.
29. Yoshida E, Watanabe T, Takata J, Yamazaki A, Karube Y, Kobayashi S. Topical application of a novel, hydrophilic gamma-tocopherol derivative reduces photo-inflammation in mice skin. J Invest Dermatol. 2006;126(7):1633-40.
30. Kamei Y, Otsuka Y, Abe K. Comparison of the inhibitory effects of vitamin E analogues on melanogenesis in mouse B16 melanoma cells. Cytotechnology. 2009;59(3):183-90.
31. Bellemare J, Roberge CJ, Bergeron D, Lopez-Vallé CA, Roy M, Moulin VJ. Epidermis promotes dermal fibrosis: role in the pathogenesis of hypertrophic scars. J Pathol. 2005;206(1):1-8.
32. Kamei Y, Otsuka Y, Abe K. Comparison of the inhibitory effects of vitamin E analogues on melanogenesis in mouse B16 melanoma cells. Cytotechnol 2009;59(3):183-90.
33. Bellemare J, Roberge CJ, Bergeron D, Lopez-Vallé CA, Roy M, Moulin V. Epidermis promotes dermal fibrosis: role in the pathogenesis of hypertrophic scars. J Pathol 2005;206(1):1-8.
This study was performed at the authors' private practice - Rio de Janeiro (RJ), Brazil.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}