


Felipe Bochnia Cerci1; Tri H Nguyen2
Keywords: MOHS SURGERY; SURGICAL FLAPS; NOSE NEOPLASMS.
The paramedian forehead flap (PFF) has been used for centuries in nasal reconstruction. It is a unique flap in terms of restoring complex nasal defects. Overtime, numerous modifications and refinements have been described to improve its outcome and versatility.1 Adequate training, good surgical technique, and careful planning are necessary to achieve optimal results.
The PFF is classified as a staged interpolation flap for having the following features: vascular pedicle based on a named artery and/or its tributaries, donor location distant and noncontiguous from the defect, and more than one stage for completion. Its main indications are large and deep wounds located on the distal nose (tip and ala).2 It can uniquely restore contour, texture, projection of the nasal tip and convexity of the ala, especially when combined with cartilage grafting. Due to its bulkiness, the PFF is less ideal for the upper nose (nasal sidewall, dorsum and root), which has thinner skin. Disadvantages related to the flap are the necessity for a multi-staged procedure and the forehead donor site scar, which is usually inconspicuous.
The purpose of this study is to evaluate the versatility of the PFF for nose reconstruction after Mohs micrographic surgery, especially in an outpatient setting under local anesthesia. Furthermore, the article will discuss traditional approaches versus more recent refinements on its design and execution.
Patients
This was a retrospective study of 19 patients whose nasal defects were repaired with the PFF after Mohs micrographic surgery. Cases were identified from a private Mohs practice from 2010 to 2013. Through chart review and by analysis of photographic documentation, the following demographic and surgical data were examined: age, gender, tumor type, defect sizes and subunits involved, number of Mohs stages and repair stages, supplementary measures for patient comfort, lining restoration, cartilage grafts, pedicle design, donor site closure, postoperative complications, smoking habits, follow-up period and outcomes.
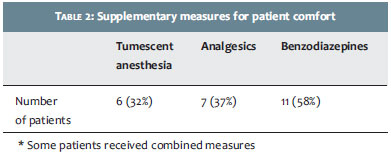
All patients signed an informed consent form prior to surgery allowing publication of photographs in scientific journals. All procedures (Mohs surgery for tumor clearance and subsequent reconstruction) occurred in an outpatient setting. Nerve blocks (supraorbital and supratrochlear) and or tumescent anesthesia supplemented local anesthesia. Prior to the procedure, patients received oral analgesics, benzodiazepines or antibiotics, if necessary. Most PFF repairs followed the Mohs surgery on the same day. Typically, the second stage took place 3 to 4 weeks after the first stage. For those that required a third stage, it was performed 3 to 4 weeks after the second.
Flap design and execution
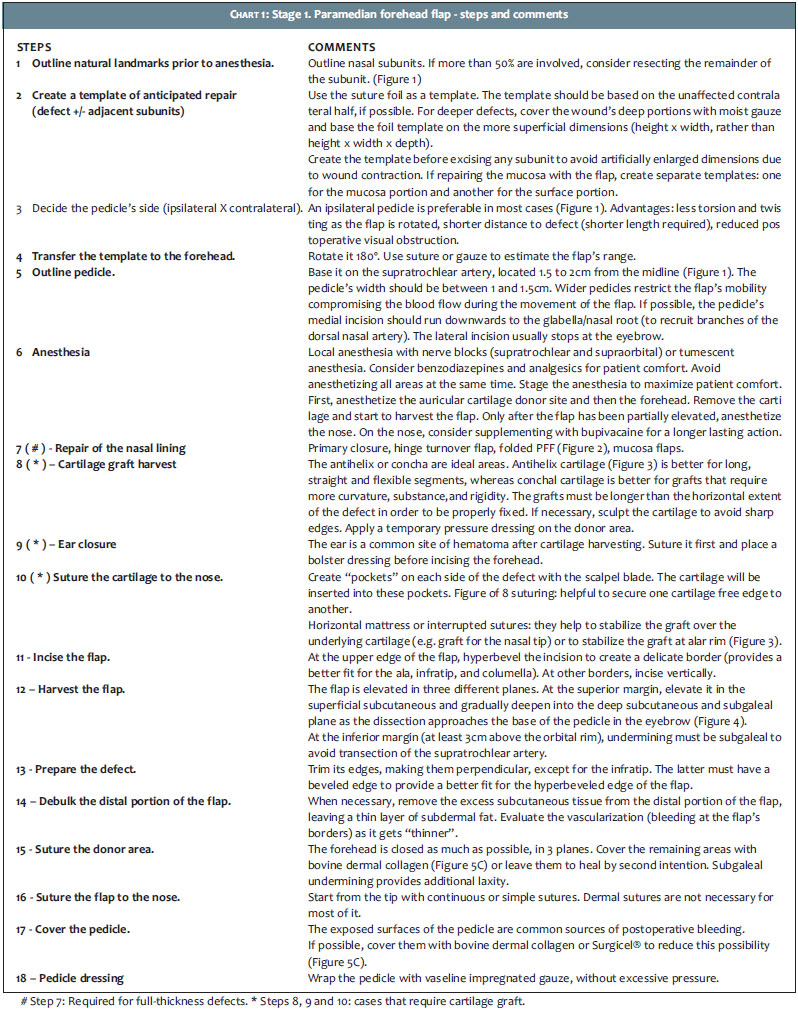
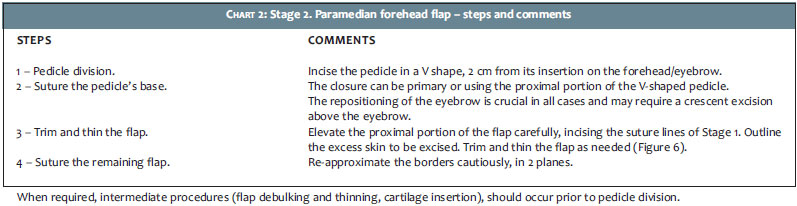
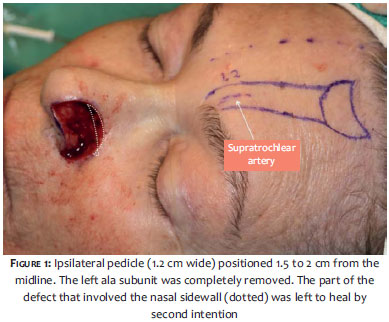
The PFF requires a substantial knowledge of anatomy, surgical planning, and surgical skill for its correct design and execution. The primary vascular supply for the PFF is the supratrochlear artery, which is located at the medial border of the eyebrow, 1.5 to 2 cm from the facial midline. Although a Doppler may help identify the artery, this is usually not necessary as the location is highly predictable. The artery emerges from the supratrochlear foramen and below the orbital rim lies deep to periorbital muscles (orbicularis oculi and frontalis). Above the rim, the artery pierces the frontalis muscle and gradually becomes more superficial, reaching the subcutis midway up the forehead. Therefore, dissection of the pedicle should be below deep fascia near the orbital rim. Secondary vascular supply to the PFF include branches from the dorsal nasal artery.3 Charts 1 and 2 describe a stepwise approach for the two-stage flap design and execution (Figures 1-6).
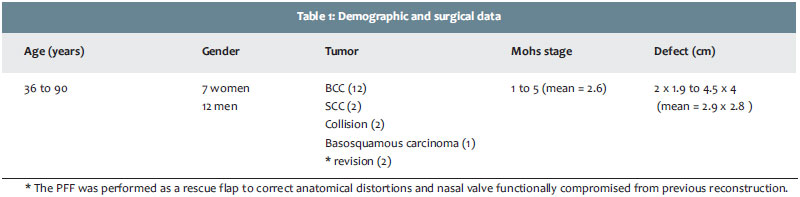
Nineteen patients were included in the study. Demographic and surgical data are shown in table 1. Age of the patients varied from 36 to 90 years (mean age, 67.1 years), with a predominance of men (12 men x 7 women). Basal cell carcinoma was the most common tumor (n=12), followed by squamous cell carcinoma (n=2), collision tumor (n=2) and basosquamous carcinoma (n=1). In two patients, the PFF was performed as a rescue flap to correct anatomic distortions and impaired nasal valve function from previous reconstructions. Most patients received either anxiolytics and or oral analgesics as adjuncts to local anesthesia during surgery (Table 2). Only one patient was a smoker.
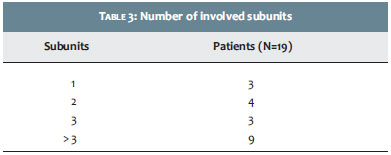
The number of Mohs stages necessary to achieve clear margins varied from 1 to 5 (mean, 2.6). Defect sizes ranged from 2 cm x 1.9 cm to 4.5 cm x 4 cm (mean, 2.9 cm x 2.8 cm). Sixteen (84%) patients had defects that involved multiple subunits (Table 3). Tip (n=15) and ala (n=12) were the most frequent involved. Resection of an additional portion of a subunit was performed in 17 (90%) patients. The PFF was combined with other closures in four patients that had wounds extending beyond the nasal subunits.
Mucosal restoration was required for full-thickness defects in 4 (22%) patients and was achieved by folded PFF (n=3) or primary closure (n=1). Structural support provided by ear cartilage was necessary in 12 (67%) patients. Cartilage was harvested from the conchal bowl (n=8) or scaphoid fossa/antihelix (n=4). A posterior incision to harvest the graft was used in 9 (75%) of the 12 patients.
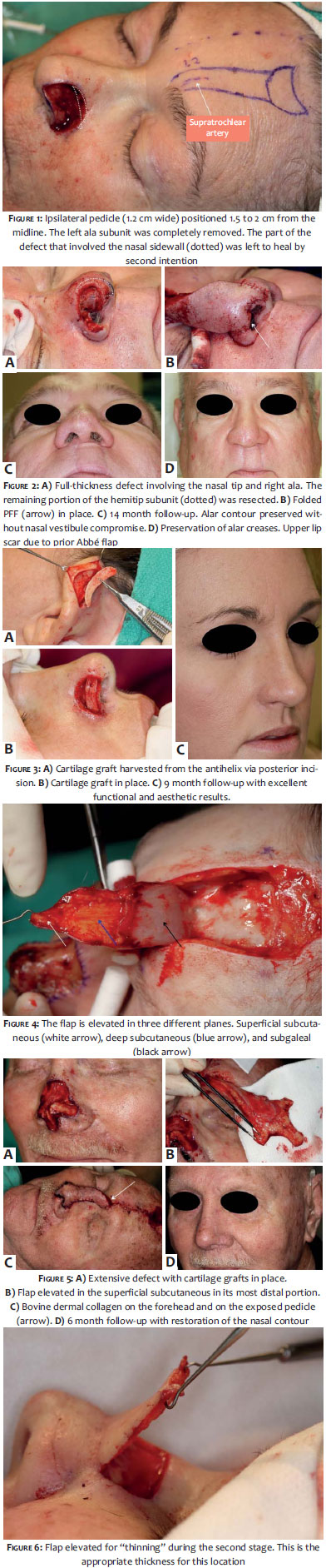
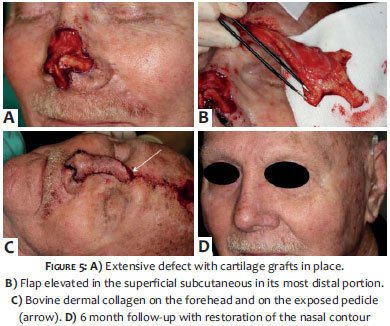
The flap pedicle was designed ipsilateral to the defect in 14 (74%) patients (Figure 1) and contralateral in 2 (10%). The three remaining patients had defects centrally located. Closure of the forehead was most commonly accomplished by primary closure combined with bovine dermal collagen (n=15) or second intention healing (n=3). Only one patient had the forehead closed completely. Bovine dermal collagen was also used in 18 (95%) patients to cover the exposed surface of the pedicle (Figure 5).
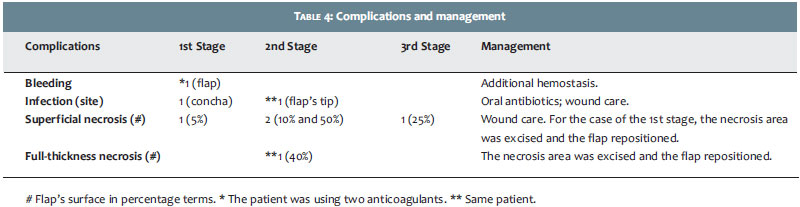
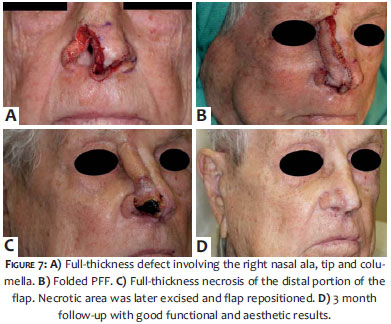
Complications were minor and uncommon (Table 4). Three complications occurred following the first stage. One patient had post-operative bleeding immediately after surgery, which required additional hemostasis for control. This patient was taking two anticoagulants. Another patient developed infection on the cartilage donor site and one superficial tip flap necrosis (<5% of flap surface). The infection was treated with oral antibiotic whereas the necrosis was excised and the flap repositioned, which required an extra stage. Following the second stage, three patients had complications. Two had superficial and proximal necrosis (10 and 40% of flap surface) due to aggressive thinning. Both were treated with wound care and healed uneventfully. One patient had full-thickness necrosis (40%) associated with infection. He was treated with oral antibiotics and excision of the necrotic area, followed by flap repositioning (Figure 7). Complication after the third stage occurred in only one patient, who developed superficial necrosis (25% of flap surface) from aggressive thinning. None of the patients who had complications were current smokers. Despite complications, all patients had excellent functional and aesthetic results. No tumor recurrences occurred after follow-up period ranging from 4 to 49 months (mean, 29 months).
The nose is one of the most common locations for skin cancer and frequently represents a challenge for reconstruction after surgical defects. Closure options are individualized for each patient and defect. For large defects on the distal nose, however, options that achieve a good functional and aesthetic outcome are limited. When wounds are extensive, deep, and or involve missing cartilage or mucosal lining, no other repair can approach the consistency and predictability of the PFF.
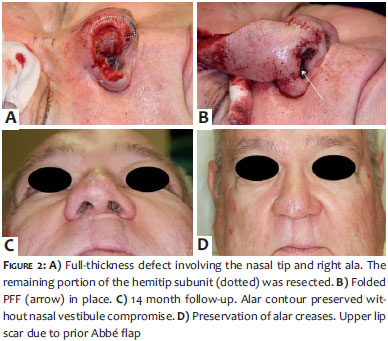
The subunit principle is an important concept in reconstruction.4 If a defect involves greater than 50% of a subunit, excising the residual skin and resurfacing the entire subunit may yield better aesthetic outcomes (Figure 1). Just as a damaged fender or car door is completely replaced for better contour and camouflage, the nose also benefits from subunit repair. This principle, however, is not absolute.5 Excellent results may be achieved with partial subunit replacement. In this study, three (16%) patients had partial subunit resections (hemitip) with excellent results (Figure 2). Fourteen (74%) patients had complete subunit excision. Among those, seven (50%) also had partial excision of an additional subunit.
The PFF should be thought of as a robust surface covering that can provide soft tissue thickness but not structural support. Nasal lining and structural cartilage are the infrastructures that must be either intact, supplemented, and or restored prior to the PFF.6 Options to restore small mucosal defects (<1cm) include a turnover hinge flap, turndown of a forehead flap extension, a full-thickness skin graft (FTSG), and bipedicle vestibular skin advancement flap. Larger lining restoration may require a turnover forehead flap, FTSG vascularized by an overlying PFF, or intranasal lining flaps (septal mucoperichondrial hinge flap, composite septal chondromucosal pivotal flap).7,8 Intranasal mucosal flaps are difficult to perform without conscious sedation or general anesthesia. Other options above, however, may be successfully executed under local anesthesia.
Cartilage grafts are either structural (native cartilage present but additional needed for support) or restorative (replacing what was removed). Structural functions of cartilage include: 1) preventing tissue contraction and distortion, 2) bracing heavy flap tissue, 3) maintaining airway patency and augmenting the internal nasal valve, and 4) achieving contour support (i.e. nasal tip graft for better projection).2 Donor sites for cartilage grafts may include the antihelix (scaphoid fossa) and the conchal bowl from one or both ears.9,10 Other cartilage sources, such as a cadaveric or patient's rib and nasal septum are beyond the scope of this article.
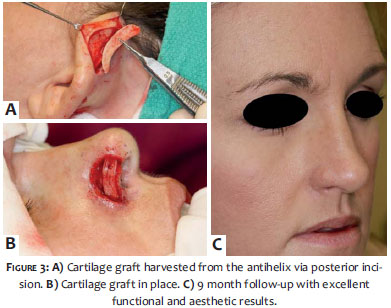
Incisions for harvesting cartilage may be either anterior or posterior. Anterior incisions are easier for access, but scars are more noticeable. Antihelical cartilage is ideal for long, straight and flexible segments, whereas conchal cartilage is ideal for grafts that demand more curvature, substance, and rigidity. Conchal grafts work better to avoid nasal valve or lobule collapse, and for collumela and tip projection. Antihelical cartilage is better suited to avoid alar rim contraction (Figure 3).9,10 Sculpting and beveling of the graft is often necessary to achieve the desired thickness, contour, shape, and tapered edges. This should be carefully done since cartilage is a fragile structure and may break during the process. Traditionally, a number 15 blade is used for sculpting. However, a schick blade allows a more delicate sculpting and graft contour if properly used. Cartilage grafts may be safely harvested under local anesthesia.11 Only one patient developed a postoperative infection, which resolved after oral antibiotics. Postoperative pain after PFF is variable. However, if cartilage grafting was performed then the auricular donor site is predictably more painful after surgery than the forehead flap donor site. Injecting long acting local anesthetic (Bupivacaine) after closing the ear donor site and postoperative analgesics (anti-inflammatory/narcotic combination) is advised for patient comfort.
Whether the PFF should be completed in two or three stages is a matter of debate. Folded PFFs that restore nasal lining absolutely require three stages (Figure 2). The first stage harvests the flap and folds it to provide both nasal lining and surface covering. The second stage (3 weeks) retains the pedicle, but opens the PFF margin at the alar rim to debulk excess tissue and to insert cartilage support. The third stage (6 weeks) divides the pedicle and sculpts the flap further for completion. PFFs that are not folded to restore lining may also be staged in 3 sessions.12 The first stage incorporates cartilage support and PFF creation and inset. The second stage (3 weeks) elevates the flap partially and debulks excess tissue to improve contour. The third stage (6 weeks) then divides the pedicle. The main advantage of the three-stage PFF is the ability to sculpt a thin, supple contour in patients with delicate nose tips and ala. Two stage flaps in these patients often result in bulbous, thick contours. Disadvantages of the three-stage PFF are the delay in pedicle division and the extra procedure. However, the three-stage procedure is more reliable in smokers as the flap contains muscle and has a very robust blood supply. It may also be of benefit in cases where a profound underlying lining and cartilaginous reconstruction have been performed, as the frontalis provide an extremely rich anastomotic vascular network.13 Six patients (31%) required a three-stage PFF in this study. Three were submitted to folded PFFs, two required a more aggressive thinning, and one needed repositioning of the flap due to distal necrosis.
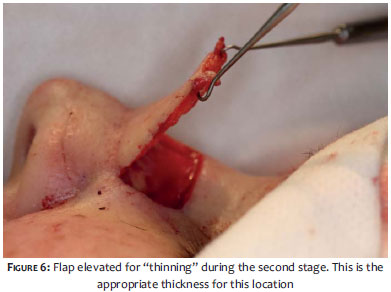
For most patients, the two-stage approach is safely performed by debulking the distal portion of the flap at the first stage. As long as a thin layer of subdermal fat is preserved, then the supratrochlear artery is protected.13 Thinning of the proximal portion of the flap is usually performed at the time of pedicle division and should be carefully done (Figure 6). If elevation and thinning are too aggressive, necrosis may result.
Pedicle side is an important consideration when designing the PFF. Traditionally, the pedicle has been designed contralateral to the defect to minimize its torsion. However, a narrow pedicle (1 to 1.5 cm) allows an ipsilateral design without concerns about significant torsion.14 Moreover, the ipsilateral design increases the flap reach. Further modifications that increase flap length include extending the incisions of the pedicle below the orbital rim,4,6,15 and extension of the flap into the anterior frontal scalp or in an oblique fashion.16 The oblique design, however, may affect the eyebrow position after donor site closure or contraction caused by second intention healing. The presence of scars within the donor site of the forehead should be assessed since it may affect the flap vascular supply.17
Attempting to completely close the forehead donor site is not advisable. The forehead is approximated as much as possible without tension. However, when significant tension is noted, the remaining wound should heal by second intention.2 Heroic measures such as bilateral forehead rotations or skin grafting only increases morbidity and pain without significant benefits. To facilitate second intention healing without the morbidity of additional procedures, bovine dermal collagen was used in 15 (79%) of our patients, an approach that has not been reported in other studies with PFF. We do not recommend the use of FTSG or STSG for the remaining donor site closure since it can result in a large "patchy scar". Recently described for the PFF, however, is a delayed FTSG harvested from the pedicle on the stage II.18
Traditionally, the non-epidermal portion of the pedicle is left exposed. However, postoperative oozing is common as epinephrine from the local anesthetic wears off. Options that reduce bleeding from the pedicle include application of a hemostatic agent (Surgicel® ),19 skin grafts12 or bovine dermal collagen. The disadvantage of a skin graft is the extra procedure required. Regardless of the method chosen, adequate hemostasis of the pedicle is a critical step.
Defects that extend beyond the nasal subunit are best closed separately (Figure 1). For instance, cheek defects are typically reconstructed with primary closure or cheek advancement flap. The leading border of the cheek flap may be secured to the periosteum of the maxilla to prevent the flap from migrating laterally during the healing process.
Potential complications of the PFF include bleeding, pain, poor scarring, infection, dehiscence, distortion of free margins and flap necrosis.20 In a recent study by Cook,21 the rate of complications associated with dermatologic surgeons performing PFF in an outpatient setting under local anesthesia was equal to or lower than published complication rates from other surgical specialties. In this study, despite the higher rate of complications compared to previous studies performed by dermatologic surgeons, complications were minor and treatable. Furthermore, all patients had optimal to excellent functional and aesthetic results.
The PFF is a valuable flap in the repair of large and deep nasal defects following Mohs micrographic surgery. Its reliable blood supply, color, and textural qualities and resultant contour warrant strong consideration for its application. Restoring the entire subunit should be considered. Optimal results, however, may be achieved with hemi subunit repair. With good surgical planning, measures for patient comfort, and meticulous technique, the PFF may be safely performed in an outpatient setting and can achieve unique restoration of the nose.
1. Mazzola RF, Marcus S. History of total nasal reconstruction with particular emphasis on the folded forehead flap technique. Plast Reconstr Surg. 1983;72(3):408-14.
2. Nguyen TH. Staged interpolation flaps. In: Roher TE, Cook JL, Nguyen TH, Mellete Jr, JR, editors. Flaps and grafts in dermatologic surgery. New York: Elsevier, 2007. p. 91-105.
3. Shumrick KA, Smith TL. The anatomic basis for the design of forehead flaps in nasal reconstruction. Arch Otolaryngol Head Neck Surg. 1992;118(4):373-9.
4. Burget GC, Menick FJ. The subunit principle in nasal reconstruction. Plast Reconstr Surg. 1985;76(2):239-47.
5. Rohrich RJ, Griffin JR, Ansari M, Beran SJ, Potter JK. Nasal reconstruction beyond aesthetic subunits: a 15-year review of 1334 cases. Plast Reconstr Surg. 2004;114(6):1405-16; discussion 1417-9.
6. Burget GC. Aesthetic restoration of the nose. Clin Plast Surg. 1985;12(3):463-80.
7. Boyd CM, Baker SR, Fader DJ, Wang TS, Johnson TM. The forehead flap for nasal reconstruction. Arch Dermatol. 2000;136(11):1365-70.
8. Baker S. Internal lining. In: Baker S, Naficy S, editors. Principles of nasal reconstruction. St Louis: Mosby, 2002 p. 31-46.
9. Ratner D, Skouge JW. Surgical pearl: the use of free cartilage grafts in nasal alar reconstruction. J Am Acad Dermatol. 1997;36(4):622-4.
10. Byrd DR, Otley CC, Nguyen TH. Alar batten cartilage grafting in nasal reconstruction: functional and cosmetic results. J Am Acad Dermatol. 2000;43(5 Pt 1):833-6.
11. Sage RJ, Leach BC, Cook J. Antihelical cartilage grafts for reconstruction of mohs micrographic surgery defects. Dermatol Surg. 2012;38(12):1930-7.
12. Menick FJ. A 10-year experience in nasal reconstruction with the three-stage forehead flap. Plast Reconstr Surg. 2002;109(6):1839-55; discussion 1856-61.
13. Burget GC, Menick FJ. Nasal support and lining: the marriage of beauty and blood supply. Plast Reconstr Surg. 1989;84(2):189-202.
14. Menick FJ. Aesthetic refinements in use of forehead for nasal reconstruction: the paramedian forehead flap. Clin Plast Surg. 1990;17(4):607-22.
15. Burget GC, Menick FJ. Nasal reconstruction: seeking a fourth dimension. Plast Reconstr Surg. 1986;78(2):145-57.
16. Angobaldo J, Marks M. Refinements in nasal reconstruction: the crossparamedian forehead flap. Plast Reconstr Surg. 2009;123(1):87-93; discussion 94-7.
17. Brodland D. Paramedian forehead flap reconstruction for nasal defects. Dermatol Surg. 2005;31(8 Pt 2):1046-52.
18. Kim SK, Park HS, Lee SC. A novel method for closing large donor defects when performing paramedian forehead flaps. Dermatol Surg. 2013;39(10):1549-50.
19. Christenson LJ, Otley CC, Roenigk RK. Oxidized regenerated cellulose gauze for hemostasis of a two-stage interpolation flap pedicle. Dermatol Surg. 2004;30(12 Pt 2):1593-4.
20. Little SC, Hughley BB, Park SS. Complications with forehead flaps in nasal reconstruction. Laryngoscope. 2009;119(6):1093-9.
21. Newlove T, Cook J. Safety of Staged Interpolation Flaps After Mohs Micrographic Surgery in an Outpatient Setting: A Single-Center Experience. Dermatol Surg. 2013;39(11):1671-82.
This study was performed at Mohs & Dermatology Associates - Northwest Diagnostic Clinic - Houston (TX), USA.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}