


Mauricio Mendonça do Nascimento1; Danielle Ioshimoto Shitara2; Sergio Yamada1
Keywords: DERMOSCOPY; HUTCHINSON'S MELANOTIC FRECKLE; KERATOSIS, ACTINIC; FACE.
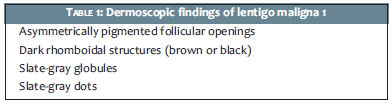
Dermatoscopic examination of pigmented lesions on the face differs from usual dermoscopy due to the absence of a pigmented network at this location. Instead, it observes a pseudonetwork, and also there are some well-established parameters for the diagnosis of lentigo maligna (LM) in the face.1 (Table 1) Pigmented actinic keratoses (PAK) on the face are usually a diagnostic pitfall in the differentiation of LM. The present article describes some cases of dermoscopic images of doubtful PAKs with LM findings, as well as typical LM and PAK findings, which may be of assistance in the differential dermoscopic diagnosis.
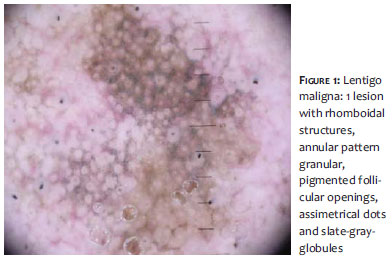
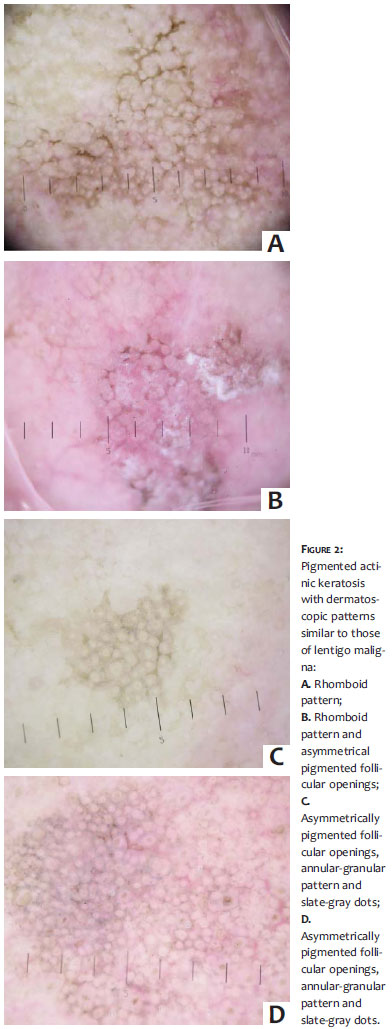
Both the LM (Figure 1) and the PAK (Figure 2) may have the same appearance, except for the dark blurs.2 The literature has described dermoscopic parameters that suggest the diagnosis of PAK rather than that of LM, with a rougher surface, due to hyperkeratosis associated with this type of lesion, the presence of multiple lesions (sign of the surroundings), a more regular architecture of the dots, hypodense holes in the pseudonetwork or the "strawberry" pattern (Figure 3).3-5 These aspects of the PAK have already been tested for their diagnostic validity against LM,4,5 with a prominent "strawberry" pattern found in the PAK, but not in the LM.4 Given that the dermoscopy consensus establishes that a single dermoscopic parameter does not allow diagnosis, it only has the potential for assisting in diagnosis. The examples of PAK described in the present article (Figure 2) indicate that the rough surface is not always present. The sign of the surroundings takes into account the fact that other keratotic lesions may be seen in the face with actinic damage, helping in the identification of the suspicious lesion, although malignant lentigines can be found in actinic skin. When the PAK does not have pigmented areas, (Figure 2) the presence of classical aspects of actinic keratosis can be of help (hyperkeratosis, reddened areas and the "strawberry" characteristic), however reddened areas arranged in rhomboidal layout around the follicle should raise suspicion of the LM diagnosis, as it has been described more recently.4 The pigmentary patterns described for the dermatoscopic diagnosis of LM 1 (Table 1) have been published with diagnostic accuracy,3-5 and therefore can provide guidance for the choice of the site to be biopsied in case of the suspicion of malignancy, however those patterns can be found in PAK (Figure 2). The examples presented show that the annular-granular pattern, as well as the slate-gray dots and globules, are possible in PAK (Figures 2 and 3). In this manner, a more regular distribution of dots and the absence of follicular openings asymmetrically pigmented are parameters that aid in the definition of PAK.5 The presence of asymmetrical openings, however, does not exclude the possibility of PAK, in which case the biopsy will define the diagnosis.
Pigmented lesions on the face present a diagnostic pitfall when it is necessary to exclude the diagnostic possibility of LM-in particular because this diagnosis has dermoscopic aspects in common with PAK, leading to unnecessary biopsies. Both lesions can be found in all areas of the face, and their distribution is similar.5 Thus, further studies are needed to validate the parameters for differentiating between PAK and LM. To date, in those cases, a skin biopsy remains the gold standard and is mandatory in order to exclude malignancy.
1. Schiffner R, Schiffner-Rohe J, Vogt T, Landthaler M, Wlotzke U, Cognetta AB, et al. Improvment of early recognition of lentigo maligna using dermatoscopy. J Am Acad Dermatol. 2000;42(1 pt 1):25-32.
2. Akay BN, Kocyigit P, Heper AO, Erdem C. Dermatoscopy of flat pigmented facial lesions: diagnostic challenge between pigmented actinic keratosis and lentigo maligna. Br J Dermatol. 2010;163(6):1212-7
3. Zalaudek I, Ferrara G, Leinweber B, Mercogliano A, D'Ambrosio A, Argenziano G. Pitfalls in the clinical and dermoscopic diagnosis of pigmented actinic keratosis. J Am Acad Dermatol. 2005;53(6):1071-4.
4. Goncharova Y, Attia EA, Souid K et al. Dermoscopic features of facial pigmented skin lesions. ISRN Dermatology. 2013;2013:546813. [Epub ahead of print]
5. Nascimento MM, Yamada,S. Almeida, F. New Dermoscopic features for the diagnosis of pigmented actinic keratosis. Dermatology 2006;212(3):290.
Study performed at the Universidade Federal de São Paulo (UNIFESP)-São Paulo (SP), Brazil.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}