


Frederico Hassin Sanchez1; Juliany Lima Estefan2; Ivan Diazgranados Fernandez3
Keywords: CARCINOMA, BASAL CELL; MOHS SURGERY; SURGICAL FLAPS.
The nasal ala is a complex structure that is part of the nasal vestibule. It has respiratory function: it filters,moistens, and warms the air-allowing it to reach the lungs in addition to assisting in the phonation process.1 This process is possible thanks to the anatomical structure of the nasal ala, which is composed of dense connective tissue and part of the alar cartilage, which provides support to it and prevents it from collapsing during inspiration (valve movement). The integrity of the nasal ala is crucial for maintaining the contour and aesthetics of the face and nose, the latter constituting one of the most prominent and central structures.
Basal cell carcinoma (BCC) is the most common malignant tumor in the world 2 and has as its main risk factor exposure to the sun.3.4 Most cases occur in photo-exposed body sites5 and its frequency in the face ranges from 27.5-91.1%.5 Its most common form of occurrence is the nodular-ulcerative type,5 which presents clinically as an erythematous-pearly papule or nodule with telangiectasias, possibly with a central ulceration.2 Its occurrence increases in the elderly.3,4 About 25.0% of BCCs occur on the nose.6 The nasal ala is exposed to ultraviolet radiation daily, resulting in a high prevalence at that site.
Several therapeutic modalities are described in the literature for the treatment of BCC. Among them, Mohs micrographic surgery (MMS) stands out for allowing a rigorous histological control of surgical margins, with a high cure rate and low recurrence rates.7
In most cases the tumors are small or superficial and do not compromise the full thickness of the nasal ala. When tumors are large, infiltrating, or recurring, the compromise can be complete, including the nasal mucosa (Figure 1) and may lead to partial or total amputation of this structure, having a great psychological impact on the patient. Its surgical reconstruction poses a challenge to the surgeon, who should prioritize the oncologic cure, preserving the functionality and aesthetic aspect whenever possible.
The present article describes a series of five cases, each involving complete amputation of the nasal ala after treatment of BCC with MMS, and which were reconstructed using the reverse Spear's nasolabial flap, also known as the "somersault" flap. The authors' objective is to describe the technique in detail, demonstrating the surgical applicability of this type of reconstruction, its advantages,difficulties, and results.
A number of techniques are described for the total reconstruction of the nasal ala, most of them including the use of cartilage grafts to allow tissue support and prevent the "valve" movement during inspiration. The flap described by Spear et al. in 1987 8-and more recently published in detail by Cook,8 allows the complete reconstruction of the nasal ala, maintaining its structural integrity without cartilage grafts and providing contour to the structure with satisfactory cosmetic results in a single surgical event. The decision to use the "somersault" flap is made based on the examination of the donor area in the nasogenian fold and cheek. This area should have enough skin for preparing the flap and for the primary closure, with minimal actinic damage. It should be thoroughly evaluated before surgery, for when it is "folded" it will end up occupying a location that is difficult to assess. Therefore, before choosing this technique, the potential for development of cutaneous neoplasms in the nasal vestibule should be considered.
The Spear's flap is prepared based on the detachment of the cutaneous flap from the nasogenian fold ipsilateral to the amputated nasal ala. A subcutaneous pedicle is left in order to take advantage of the vascularity of that region (described by Hebert8), which is supplied by the angular artery (Figure 2). The proximal third of the flap is lifted in the alar base and the proximal skin is used to reconstitute the interior area of the nasal ala, with its edges sutured to the remaining tissues of the nose. The distal 2/3 of the flap is folded over itself, reconstituting the free border and the external part of the nasal ala. Intradermal suture is carried out between the two parts of the flap, and the external part is adjusted so as to cover the entire surgical defect. The border of the flap is adjusted and sutured and the primary closure of the donor area is carried out. Nasal packing is recommended for 15 days in order to provide support for the shape of the nasal ala and prevent the retraction of the flap.8,9
All cases selected by the authors involve tumors of the nasal ala that were operated on at a MMS specialist center from July 2010 to April 2012.
During this period, 15 patients who presented with perforation of the mucosa and a transfixing of the entire thickness of the nasal alaunderwent surgery. Of these, 10 presented loss of the distal part (free border), corresponding to a complete amputation; 5 underwent surgical reconstruction with Spear's flap and were therefore selected for the present study.
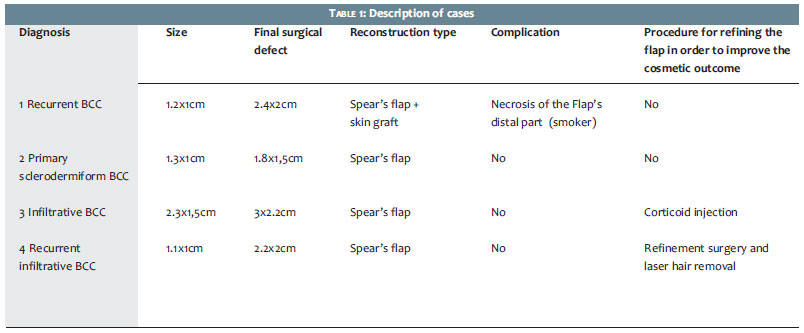
Two patients had lesions that extended beyond the nasal ala (Figure 3), and therefore underwent other complementary methods for closing the surgical wound. In threecases, the authors recommended subsequent procedures for the refinement of the flap in order to achieve a better cosmetic result (Table 1). One of the patients had beard hairs transferred with the flap and was referred for laser epilation post-operatively.
In cases requiring a second surgical event, the authors aimed at correcting the asymmetry of the nasal alae, caused by the greater thickness of the flap. In one patient,thisthickening was corrected with direct corticosteroid infiltration into the flap.
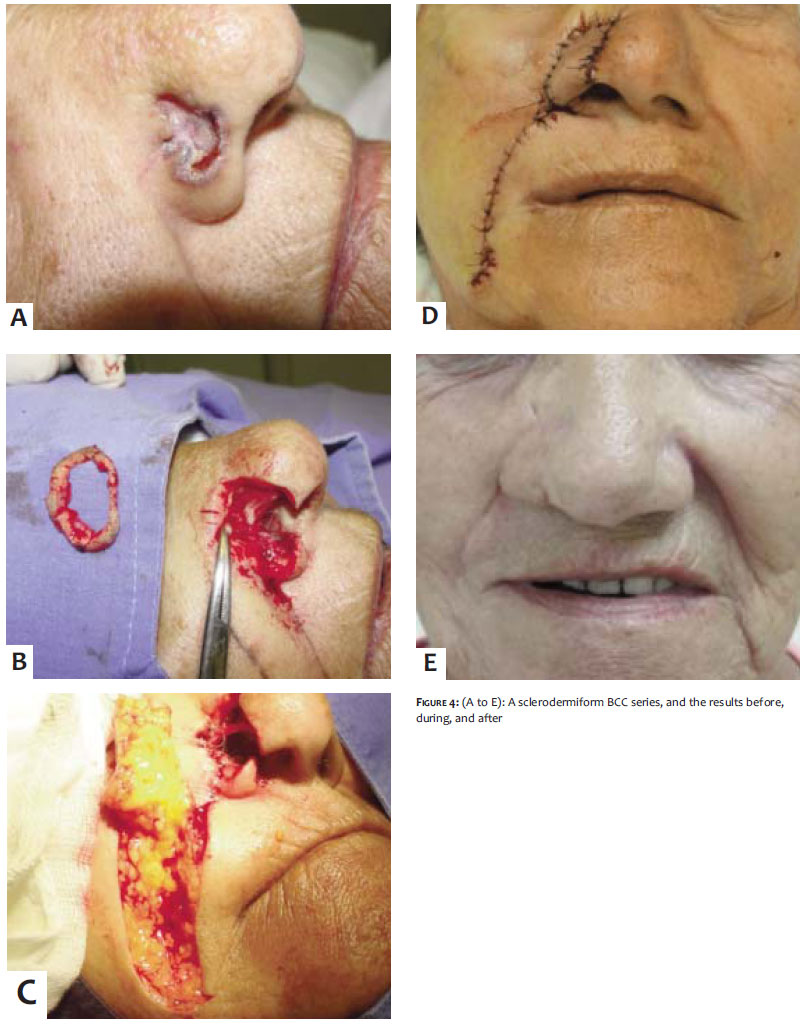
All patients had their nasal ala function preserved, and none showed the "valve" phenomenon during inspiration (Figure 4).
BCC is a common tumor in the nasal ala. MMS is the method of choice for the treatment of invasive or recurrent tumors in this region. Amputation of the nasal ala may be required for the complete excision of the tumor, resulting in a difficult to correct surgical defect.
The Spear's flap allows the complete reconstruction of the nasal ala, maintaining its structural integrity and providing contour to the nasal ala with satisfactory cosmetic results. Although this reconstruction was originally described as a single surgical event, in some cases a second procedure is indicated for refining the flap and improving the aesthetic outcome.
Given the complexity of the surgical defects, the cosmetic outcome was already deemed satisfactory in the studied patients by the first surgical event-even in the cases that underwent a second procedure for refinement.
The complete reconstruction of the nasal ala is a challenge, and the Spear's flap is a good option for ensuring structural integrity to the tissue and for preventing the "valve" movement without need for a cartilage graft, and in addition it confers satisfactory cosmetic resultsaftera single surgical event.
1. Kernahan DA. Reconstruction of the nose. In: Grabb W, Smith's J. Plastic Surgery - A Concise Guide to Clinical Practice. 2nd ed. Boston: Little, Brown and Company; 1973.
2. Basal Cell Carcinoma Treatment Options and Prognosis, a Scientific Approach to a Common Malignancy. Kuijpers DIM., Thissen MRTM, Neumann, MHA. Am J Clin Dermatol 2002;3(4):247-59.
3. Stanley J, Miller MD. Biology of basal cell carcinoma (part I). J Am Acad Dermatol. 1991;24(1):1-13.
4. Stanley J, Miller MD. Biology of basal cell carcinoma (part II). J Am Acad Dermatol. 1991;24(2):161-75
5. Mantese SAO, Berbert ALCV, Gomides MDA, Rocha A.Carcinoma basocelular - Análise de 300 casos observados em Uberlândia - MG. An Bras Dermatol. 2006;81(2):136-42.
6. Lebwohl MG, Heymann WR, Berth-Jones J, Coulson I. Treatment of Skin Disease. Elsevier, 2010. p. 78-82.
7. Cirurgia micrográfica de Mohs. Reis NA, Azevedo LCM, Stolf HO, Nouri K, Kimyai-Asadi A, Goldberg LH. Surg Cosmet Dermatol. 2011;3(3):227-31.
8. Iwao F. Alar Reconstruction with Subcutaneous Pedicled Nasolabial Flap: Difficulties, Considerations, and Conclusions for This Procedure. Dermatol Surg. 2005;31(10):1351-4.
9. Lin J, Tan X, Chen X, Lin J, Shi S, Tian F, et al. Another Use of the Alar Cartilaginous Flap. Aesth Plast Surg. 2006;30(5):560-563.
Study performed at the Centro de Cirurgia Micrográfica do Rio de Janeiro-Rio de Janeiro (RJ), Brazil.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}