


Barbara Lima Araújo Melo1; Lara Lima Araújo Melo2; Igor Santos Costa3; Ruana Moura Rocha4; Régia Maria do Socorro Vidal do Patrocínio5
Keywords: GENITAL NEOPLASMS, FEMALE; VULGAR NEOPLASMS; VULVAR DISEASES; PAGET DISEASE, EXTRAMAMMARY.
In 1874, Sir James Paget described a breast disease with a very particular histopathology, which was individualized two years later by Butlin. In 1889, Cracker found this very characteristic alteration in a lesion on the scrotum, calling it extramammary Paget's disease.1
Extramammary Paget's disease (EMPD) is a rare group of cutaneous neoplasias. It affects both genders, the vulva being the most affected site, followed by the perianal region, perineum, scrotum, and axilae. There are rare reports of the condition in the thighs, buttocks, eyelashes, and external ear.2,3 It typically occurs in patients 60 to 80 years of age, mainly affecting postmenopausal Caucasian women. In Asian populations, however, men are more affected.4
Clinically, the most common symptom is pruritus, and it is evidenced through erythematous, desquamative, and eczematous lesions. It is a slow growing neoplasm in which the appearance of old lesions can be modified by trauma, repeated abrasions, or secondary infection.5 Due to its nonspecific appearance, it can be mistaken for other dermatological conditions-such as psoriasis, contact dermatitis, squamous cell carcinoma, amelanotic melanoma, and mycosis fungoides-delaying diagnosis.2,3
The standard treatment for EMPD is local surgical exeresis with a 1 cm margin of normal skin, associated with inguinal lymphadenectomy.6 Due to high recurrence rates, which range from 16-50%, 7 other therapeutic options, such as Mohs micrographic surgery, photodynamic therapy, radiotherapy, and more recently immunotherapy with imiquimod, have been proposed.8 Regardless of the treatment option, it is crucial to follow up with the patient to detect possible recurrence of the disease as early as possible.
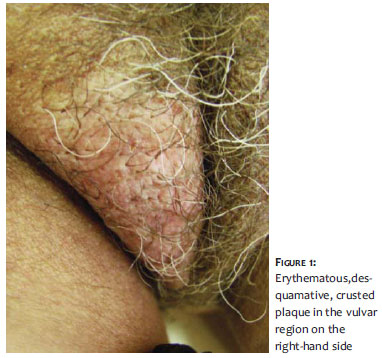
A seventy-two-year-old mulatto female patient sought medical attention in February 2010, reporting a vulvar lesion with pruritus, which onset eight years earlier. She reported the use of various topical corticosteroids without improvement. On physical examination, an erythematous, desquamative, crusted, and poorly delimited plaque could be observed in the vulvar and perineal region, on the right hand side of each. There were no palpable lymph nodes in the inguinal region (Figure 1).
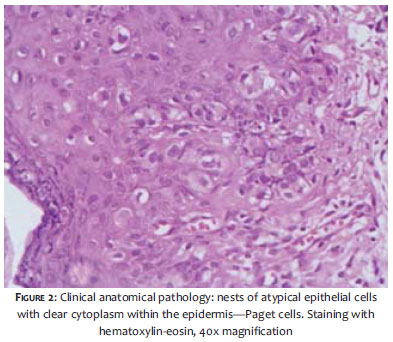
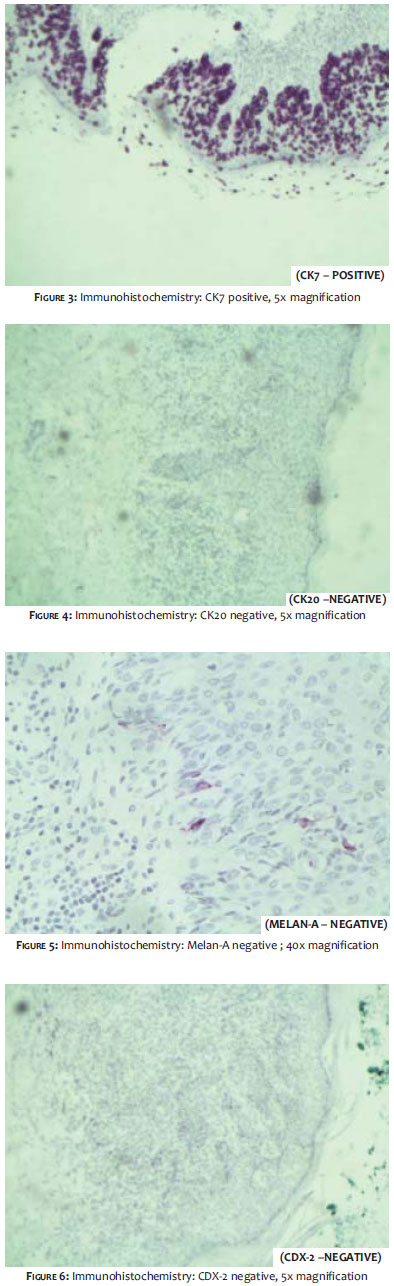
The main diagnostic hypotheses were EMPD and chronic eczema. A biopsy of the vulvar region was then carried out, with the histological (Figure 2) and immunohistochemistry (Figures 3-6) studies confirming EMPD. The thorax radiography, the bilateral mammography, and the abdominal ultrasonography showed no abnormalities.
In September 2010, a vulvectomy was performed on the right hand side, with complete excision of the lesion and superficial inguinal lymphadenectomy. No signs of residual tumor were observed in the post-operative examinations. The patient remains in regular follow up every six months, with no signs of recurrence to date.
The occurrence of EMPD corresponds to less than 2% of vulvar neoplasias. 5 The patient's epidemiological characteristics are aligned with the literature's data: female, 72-years-old and postmenopausal. The 8-year clinical history of symptoms confirms the slow progression of the neoplasia, while pointing out the difficulty of diagnosis and appropriate management of the disease.
The present case demonstrated a rare and unilateral form of vulvar EMPD, confirmed through biopsy and followed by histological analysis, which showed numerous foci represented by atypical cells with large, pale cytoplasm containing large nuclei with distinct nucleoli, extending across the mucosal epithelium in a pagetoid pattern. The immunohistochemistry revealed positivity for cytokeratin 7 (CK7), a sensitive marker, however not specific for EMPD. Negativity to that marker is rare, generally occurring in association with malignancy in internal organs.9 Negativity was also observed for cytokeratin 20 (CK20), Melan-A and CDX-2. Positive CK20 is more commonly present in EMPD associated with carcinoma,9 therefore the negativity of this marker in the studied case suggests the absence of other neoplasms. In this context, the expression pattern of cytokeratins provides a clue about the presence or absence of internal malignancy. Melan-A is a melanocyte's differentiation marker, and its negativity practically excludes the presence of amelanotic melanoma. CDX-2 is found when there is a colorectal tumor, being relevant in the diagnosis of other associated neoplasias.
EMPD generally remains restricted to the epidermis, rarely spreading via the lymphatic system.10 Subjacent malignancy ranges from 12-33% of cases, anatomically correlating to the sites of the lesions and neoplasias, with investigation being fundamental to detect internal malignancy.
Being a rare disease, little is known about the most effective treatment, and the standard approach is surgical excision with anatomopathologic evaluation of frozen margins.6 The recurrence rate after surgery is high, occurring on average after 30 months. The patient continues on a semiannual clinical follow-up, remaining asymptomatic to date. The present case suggests a good prognosis due to the presence of pagetoid cells restricted to the epidermis, and for not presenting lymph node metastases-the two main criteria for prognostic evaluation.
Due to the rarity of the case, dermatological knowledge for early diagnosis, attention to other concomitant neoplasia, and the choice of appropriate treatment-whether medical or surgical-are crucial.
1. Neto MPO. Doença de Paget Extramamária. An Bras Dermatol. 1980;55(4):183-6.
2. Shepherd V, Davidson EJ, Davies-Humphreys J. Extramammary Paget's disease. BJOG. 2005;112(3):273-9.
3. Appert DL, Otley CC, Phillips PK, Roenigk RK. Role of multiple scouting biopsies before Mohs micrographic surgery for extramammary Paget's disease. Dermatol Surg. 2005;31(11 pt 1):1417-22.
4. Chang YT, Liu HN, Wong CK. Extramammary Paget's disease: a report of 22 cases in Chinese males. J Dermatol. 1996;23(5):320-4.
5. Lloyd J, Flanagan AM. Mammary and extramammary Paget's disease. J Clin Pathol. 2000;53(10):742-9.
6. Wang X, Yang W, Yang J. Extramammary Paget's disease with the appearance of a nodule: a case report. BMC Cancer. 2010;10:405.
7. Zampogna JC, Flowers FP, Roth WI, Hassenein AM. Treatment of primary limited cutaneous extramammary Paget's disease with topical imiquimod monotherapy: two case reports. J Am Acad Dermatol. 2002;47(4 Suppl):S229-35.
8. Berman B, Spencer J, Villa A, Poochareon V, Elgart G. Successful treatment of extramammary Paget's disease of the scrotum with imiquimod 5% cream. Clin Exp Dermatol. 2003;28(Suppl 1):36-8.
9. Lundquist K, Kohler S, Rouse RV. Intraepidermal cytokeratin 7 expression is not restricted to Paget cells but is also seen in Toker cells and Merkel cells. Am J Surg Pathol. 1999;23(2):212-29.
10. Hartman R, Chu J, Patel R, Meehan S, Stein JA. Extramammary Paget disease. Dermatol Online J. 2011;17:4.
This study was performed at a private clinic-Fortaleza (CE), Brazil.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}