


Carlos Roberto Antonio1; Marina Garcia Nicoli2
Keywords: ACNE VULGARIS; CICATRIX; HYALURONIC ACID.
Acne scars represent a major complaint in the dermatologist's office. In the past, the management of such scars was a challenge; nowadays, there are many treatment options.
According to their characteristics, acne scars can be classified into elevated, dystrophic, and depressed.1 Depressed scars can be subdivided into distensible (where significant improvement can be observed with almost complete disappearance when the skin is stretched) and non-distensible (where no improvement is observed when the skin is stretched). In turn, distensible scars can be retractable (they present moderate fibrosis when strained) or non-retractable (without fibrosis).1
The best treatment option for non-retractable distensible scars is cutaneous filling. Retractable distensible scars are treated through a process called subcision, in which fibrous bands beneath the scar are ruptured by using needles with cutting tips.2 The treatment can be supplemented with hyaluronic acid filling and/or fractional lasers. Hyaluronic acid, a natural polysaccharide, is a component of the connective tissues of all mammals.3 It has a similar chemical structure in all species and a minimum potential for immunologic reactions.4 Due to the fact that it is natural and degrades gradually, problems associated with rejection and granulomatous reactions are rare, and it can be easily dissolved using hyaluronidase.5
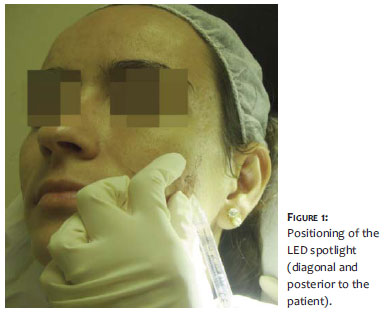
By treating non-retractable distensible acne scars with hyaluronic acid, it is possible to verify that the presence of light has an influence on their visualization. These lesions become more evident if a spotlight is positioned diagonally and posteriorly to the patient. An LED (Light Emitting Diode) is a semiconductor electronic component that converts electrical energy into light-unlike other types of lamps that use ultra-violet metallic filaments, radiation, or gas discharge. The light emitted by LEDs is intense and cold. In addition to its effectiveness, the great usefulness of LEDs in dermatology is linked to the fact that they do not cause warming either of the skin of the treated area or in the professional who is applying it.6
Thus, the present study was aimed at verifying the efficacy of the use of LED lighting in order to improve the results of filling procedures. In this way, a spotlight positioned diagonally and posteriorly to the patient during the procedure, allows for a better visualization of the shadows and reliefs of scars. As a result, it was possible in fact to note an enhancement in the visualization of the appearance of the scars. The observation started under regular yellow lighting, which was then replaced by LED lighting.
There are no reports in the literature regarding the use of this device to assist the treatment of distensible scars.
From March 2008 to May 2010,12 patients with depressed, distensible, non-retractable acne scars were recruited for the present prospective comparative study that was performed within the ethical standards regulated by the Declaration of Helsinki.
Smokers, those on anticoagulants, or those with elevated or non-distensible scars were excluded.
The treatment was performed exclusively using intradermal injections of monophasic reticulate crosslinked hyaluronic acid in the concentrations of 24 mg/ml and 25 mg/ml. Scars on both sides of the face were treated, in the following sequence:
- application of filling substance with the visualization of scars under yellow light from a diagonal and posterior position, followed by the evaluation of the corrected scars
- application of filler substance with the visualization of scars under LED lighting from a diagonal and posterior position, followed by the evaluation of the corrected scars
Photographic records were made in standardized positions-frontal and 45º and 90º profiles-with the same camera, before and after the two applications.
The evaluation of results was carried out through questionnaires completed by patients who attributed a percentage of improvement (in parameters from 0 to 100, gradations of 5%) for the scars treated without LED lighting (during the procedure) and with the assistance of LED lighting (immediately after application).
In addition, two physicians not related to the study evaluated the percentage of improvement during the procedure without LED lighting and immediately after application with LED lighting. The degree of improvement of distensible scars was classified as excellent (76-100%), good (51-75%), moderate (26-50%), or poor (0-25%).
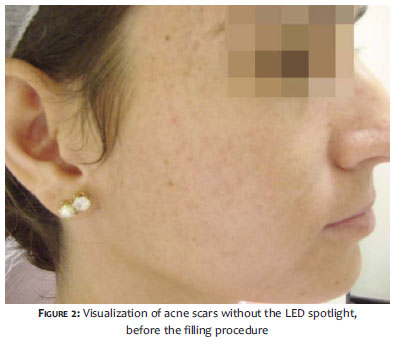
The positioning of the LED spot lighting (diagonal and posterior to the patient) is shown in figure 1. Figures 2 and 3 illustrate the visualization of acne scars without the spot and with the LED lighting spot before the filling procedure, respectively. Figures 4 and 5 show, respectively, the visualization of acne scars after the filling procedure, without the spot and with the LED lighting spot. It is possible to note that the use of the spot in this positioning provides better visualization of the areas that need correction.
In the present study, the percentage of improvement obtained was higher when the scars were treated with the assistance of LED lighting. Only one patient did not notice the difference between the treatments with and without LED. None of the patients assigned a higher degree of improvement to the treatment without the LED.
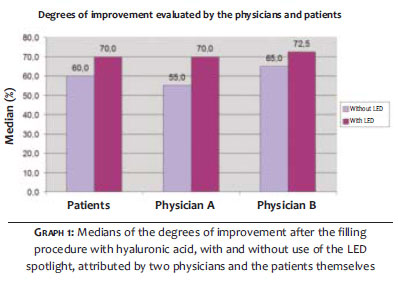
The median of the percentages of improvement attributed by patients after the treatment without the use of LED lighting was 60%. Using LED, the median of the percentages of improvement was 70%. The median of percentages of improvement evaluated by the physicians after the treatment without LED lighting was 55% (Physician A) and 65% (Physician B); after the treatment with LED lighting, the medians were 70% (Physician A) and 72.5% (Physician B). This data is illustrated in Graph 1.
The obtained percentages of improvement were categorized as excellent, good, moderate, and poor outcome. One patient (8.3%) rated the outcome of the filling with hyaluronic acid without LED as excellent, 6 patients (50%) classified it as good, 4 (33.3%) as moderate, and 1 (8.3%) as poor. After the treatment using LED lighting, 5 patients (41.7%) rated the outcome as excellent, 6 (50%) as good, and 1 (8.3%) as poor.
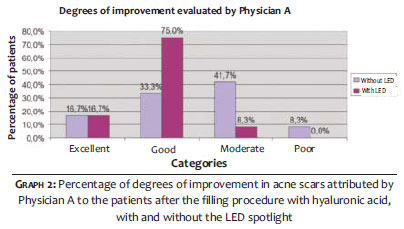
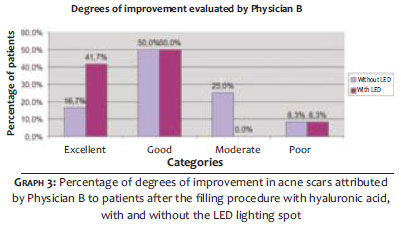
Regarding the degree of improvement attributed by the physicians, Physician A (Graph 2) rated the outcome of the filling with hyaluronic acid without LED as excellent in 2 patients, good in 4, moderate in 5, and poor in 1 patient. After the treatment with the LED spotlight, Physician A rated the outcome as excellent in 2 patients, good in 9, and moderate in 1 patient. In turn, Physician B (Graph 3) evaluated the outcome without LED light as excellent in 2 patients, good in 6, moderate in 3, and poor in 1 patient. The outcome of the treatment using LED was rated by Physician B as excellent in 5 patients, good in 6, and poor in 1 patient.
The treatment of acne scars constitutes a challenge,6-8 and the correct classification of the latter determines the success of the first. Distensible scars respond to hyaluronic acid fillings with excellent outcomes, however many are not adequately visualized due to inadequate lighting during the procedure.
The authors evaluated the perception of improvement of acne scars (distensible and non-retractable), represented by percentages of improvement in 12 patients treated with hyaluronic acid filler, in two stages: firstly without the use of LED, and secondly, with the use of a diagonal and posterior spot of LED lighting during the application. The outcomes show that the percentage of improvement was greater in the group treated with an LED spotlight. The satisfaction of patients with cutaneous filling procedures can be 90% when the indication is criterious. 6 LED lighting facilitates the application in the correct location, as lesions presenting distensibility or depression are better-and sometimes only-visualized when subjected to diagonal lights that promote shade.
The use of diagonal lighting with LED enables an accurate and detailed view of the scars, optimizing the outcome and promoting a higher patient satisfaction rate.
1. Kadunc BV, Trindade de Almeida AR. Surgical treatment of facial acne scars based on morphologic classification: a Brazilian experience. Dermatol Surg. 2003;29(12):1200-9.
2. Orentreich DS, Orentreich N. Subcutaneous incisionless (subcision) surgery for the correction of depressed scars and wrinkles. Dermatol Surg. 1995;21(6):543-9.
3. Frank P, Gendler E. Hyaluronic acid for soft tissue augmentation. Clin Plast Surg. 2001;28(1):121-6.
4. Matarasso SL, Carruthers JD, Jewell ML, Restylane Consensus Group. Consensus recommendations for soft-tissue augmentation with nonanimal stabilized hyaluronic acid (Restylane). Plast Reconstr Surg 2006;117(3 Suppl):3S-34S, discussion 35S-43S.
5. Hedén, P, Sellman G, Wachenfeldt M, Olenius M, Fagrell D. Body shaping and volume restoration: The role of hyaluronic acid. Aesth Plast Surg. 2009;33(3):274-82.
6. Vedamurthy, M, Vedamurthy, D. Dermal fillers. In: Seghal VN, editor. Dermatologic Surgery made easy. New Delhi: Jaypee Brothers Medical Publishers; 2008. p.118.
7. Metelmann U, Machado Filho CA, Meireles SIFC, Teixeira LPVB. Técnica de Croll: cirurgia de reconstrução com laser localizado em cicatrizes de acne. Surg Cosmet Dermatol. 2010;2(4):336-9.
8. Rosas FMB, Mulinari-Brenner F, Helmer KA. Comparative assessment of CO2 fractional laser and dermabrasion in the treatment of acne scars. Surg Cosmet Dermatol. 2012;4(4):298-303.
Study performed at the Faculdade de Medicina de São José do Rio Preto (FAMERP)-São José do Rio Preto (SP), Brazil.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}