


Magda Expósito de Oliveira1; Meire Gonzaga1; Marisa Gonzaga da Cunha2; Ayrton Roberto Pastore3; Carlos A. Machado4
Keywords: SKIN AGING; MESOTHERAPY; ULTRASONOGRAPHY.
Skin aging is a multifactorial process,1 classically divided into intrinsic aging (genetically determined and caused by cellular degeneration that occurs progressively from birth as the result of genetic, 2,3 hormonal 4,5 and environmental1 factors) and extrinsic aging (which is called photoagingand is caused by the cumulative results of various effects, in particular chronic exposure to ultraviolet (UV) radiation 1 but also other factors such as smoking, pollution, infrared radiation, and poor nutrition).6
UV radiation produces a sequence of alterations in the skin layers, starting with DNA damage and culminating with the fragmentation of collagen and other extracellular matrix proteins. In the epidermis, it causes damage to DNA, proteins, and lipids, interfering with cell growth and differentiation through the activation of various cell surface receptors.1 Such damage can lead to acute and transient responses (such as inflammation, formation of sunburn cells, and pruritus) but also delayed chronic responses (such as photodamage, immunosuppression, and carcinogenesis).1 Chronic alterations are clinically manifested through dryness and pigmentation and keratinization changes. The flattening of the dermal-epidermal junction reduces epidermal nourishment and hydration.7
The particles resulting from the fragmentation of collagen and other extracellular matrix proteins, promote the synthesis of metalloproteinases (MMPs), which exacerbate the damage to the ground substance.8 As a result, they cause epidermal and dermal alterations, affecting cellular components and the extracellular matrix with the loss of collagen fibers and the accumulation of disorganized elastic fibers. The activation of MMP enzymes, especially collagenase, is responsible for alterations in the collagen, as well as direct aggression to fibroblasts, with the interruption of the synthesis of new collagen.1,2 Free radicals also play an important role in cutaneous aging.1,2 Oxidative stress is caused by an imbalance between the formation of free radicals-which is caused by oxygen metabolism-and the action of antioxidant defense systems.
Free radicals damage cell structures such as membranes, DNA segments, collagen, and elastic fibers. The accumulation of these molecular alterations, particularly in proteins, constitutes the basis of cellular aging2 and results in the clinical signs of photodamage, such as a decrease inthe skin's thickness, appearance of fine wrinkles, loss of elasticity, vascular fragility, and pigmentary and keratinization alterations.1 Enzymes that minimize oxidative damage are the superoxide dismutase, catalase, glutathione peroxidase, glutathione transferase, peroxidases and thiol-specific antioxidant enzymes. Combined with low molecular weight compounds (such as ascorbate, glutathione, beta-carotene, alpha-tocopherol, bilirubins and uric acid), they serve as free radical sweepers.2
Water is essential for cellular functions and plays a key role in the differentiation process, desquamation, and final appearance of the skin. The factor that allows skin to stay healthy, with flexibility and elasticity, is the balance that exists in the hydration mechanism and in the body's ability to promote cell renewal. The small loss of water that occurs in the deeper layers hydrates the more superficial layers, facilitating enzymatic reactions that allow the maturation of the stratum corneum (EC). The concentration of water in the deep epidermis depends on the patient's age, anatomical location, and the time of year (season). Maintenance of the water gradient across the epidermis is regarded as the basic and fundamental measure in anti-aging treatment.9
The maintenance of the EC's optimum level of hydration depends on several factors. One of the most important is a complex mixture of soluble compounds in low molecular weight water, formed by amino acids, which result fromthe protein degradation of corneocytes, whose composition is regulated by the level of epidermal hydration.10 They are referred to as the natural moisturizing factors (NMF).
Cutaneous hydration is also maintained by the presence of the ground substance in the dermis. The ground substance is composed of glycoproteins and proteoglycans, including hyaluronic acid, which is a glucosamine polysaccharide synthesized in the cell membranes of the fibroblasts and eliminated into the extracellular medium, where it plays an important role in maintaining hydration, in cutaneous filling, in the modulation of inflammatory cells and the sweeping of free radicals, through the maintenance of intercellular hydric balance.10
Therefore, as a result of the oxidative process induced by UV radiation and intrinsic aging, alterations of the components of the connective tissue occur (such as a reduction in the number and activity of fibroblasts, with consequent reduction and disorganization of collagen and elastin fibers), in addition to a decrease in hyaluronic acid. Such alterations are responsible for many of the morphological and mechanical alterations that result in the formation of fine wrinkles, loss of elasticity, dryness, loss of skin tone and strength.
One of the proposed treatments for improvement of fine wrinkles, brightness, firmness, hydration, and overall appearance of the skin is the application of the compound NCTF 135 HA (registered in ANVISA, the Brazilian National Health Surveillance Agency, under the number 80279420034), which contains 12 vitamins (ascorbic acid, biotin, pantothenic acid, folic acid, inositol, nicotinamide, pyridoxine, riboflavin, thiamine, tocopherol, retinol); 23 amino acids which act directly on the synthesis of collagen and elastin (alanine, arginine, aspartic acid, asparagine, glutamine, glutamic acid, cystine, glycine, histidine, hydroxyproline, proline, lysine, leucine, serine, taurine, and others); 6 minerals which act in hundreds of enzymatic reactions and are essential to cellular function (calcium and potassium hydrochlorides, magnesium sulfate, sodium acetate, sodium hydrochloride, sodium dihydrogen phosphate); 6 coenzymes which act as biochemical activators and increase the rate of tissue repair (TPP, CoA, FAD, NAD, NADP, UTP and dinucleotide phosphatase); 5 nucleic acids which regulateand command protein synthesis; glutathione, which is a reduction agent; and hyaluronic acid (5mg/ml), with a hygroscopic action that secures large amounts of water.
Vitamins A, C, E, and B complex are important in the regulating and sweeping of free radicals, as enzyme cofactors in the synthesis of collagen, skin hydration, and also for controlling the overproduction of melanin.11-19 Ascorbic acid (vitamin C) is essential in the synthesis of collagen and participates in the regeneration of the tocopherol (vitamin E) system, helping to maintain the plasma antioxidant capacity.15 Vitamin E protects the membrane lipids from oxidation.11 Vitamin K acts on microcirculation and acts as a ligand for receptors.18 It also contains amino acids and polynucleotides that promote hydration and stimulate fibroblast activity. Sodium, potassium, calcium and magnesium act as catalysts for many enzymes. Organic silicon induces collagen synthesis.19 Non cross-linked hyaluronic acid, although somewhat unstable and with a short half-life, acts as an epidermal20 and dermal moisturizer and can stimulate its own biosynthesis through fibroblasts, which explains its longer lasting effect.21
Application through an intradermal route, known as intradermotherapy, is a medical procedure introduced in France by Pistor in 1958. It is a way of administering substances with well-established mechanisms of action, in low doses, directly in the area being treated, without significant side effects.22 It has beenused safely in Europe for over 30 years with good results. In this particular case, it involves the application of biocompatible and absorbable substances, with already established effects, necessary in the sweep of free radicals, dermal hydration, and for the elaboration of the extracellular matrix components by fibroblasts.
Therefore, intradermotherapy with the described product is indicated in cases of mild to moderate histological aging, both intrinsic and photoaging based, and as a preventionfor cutaneous aging. It is contraindicated for the treatment of expression wrinkles and as an isolated treatment for anatomical facial aging, where it can be used as an adjuvant therapy.
A monocentric, retrospective, non-comparative, open clinical study was carried out at the Cosmetic Dermatology Ambulatory of the Dermatology Discipline, at the Faculdade de Medicina do ABC, Santo André (SP), Brazil, with the aim of evaluating the efficacy of the treatment for skin rejuvenation with a combination of antioxidants, vitamin complexes, amino acids, coenzymes, and noncross-linked hyaluronic acid. The treatment was carried out in five superficial and deep intradermal applications of the product, with intervals of 15 days between the first three sessions and of 1 month between he last two sessions. The study was conducted in accordance with the ethical principles originating from the Declaration of Helsinki.
Inclusion criteria
Thirty female patients aged 40-55 years, with signs of mild to moderate photoaging were assessed. Following the routine of the Institution's Dermatology Service, all signed the Free and Informed Term of Consent (FITC), after receiving a full explanation about the product. The selected patients used only sunscreen during the treatment period.
Exclusion criteria
Exclusion criteria for the study were menopause, pregnancy, breast-feeding, bleeding disorders and use of anticoagulants, history of allergic reactions to the formulation's components, and systemic or cutaneous diseases that could interfere with the evaluation of the effectiveness of the product.
Photographs of each patient were taken from the frontal position, and right (R) and left (L) profiles for posterior comparison; patients answered a questionnaire about the perceived quality of the skin through self-assessment, including parameters such as brightness, hydration, firmness, fine wrinkles, and overall appearance, with factors ratedfrom 0 to 10; the physician applying the product also answered a predetermined questionnaire aimed at assessing those parameters, also with scores from 0 to 10; the patients underwent an ultrasound examination of skin from various regions of the face, always performed by the same physician, in a laboratory specializing in radiology (Laboratório Cetrus, unidade SãoPaulo (SP), Brazil), with a 18MHz linear transducer (Mylab 40TM-Esaote, Italy).
Application technique
After a thorough cleaning, the entire face was treated using an intradermal route, with a combination of techniques: a) point-to-point technique (1ml), with spaces of about 5mm between them, penetrating 2-4mm; b) nappage technique, where multiple punctures are performed rapidly, superficially and close to one another (1ml); and c) deep intradermal technique with 30G1/2 needle, at 4-7mm from the surface, injecting 0.01ml per point in the nasogenian folds and mandibular regions (1ml).
Five applications were performed (Days 0, 15, 30, 60 and 90), always followed by advice to the patients not to use any topical product for at least two hours.
Evaluation
Fifteen days after the last session, two questionnaires were issued again: one assessing the perceived clinical effectiveness, to be answered by the physician applying the product and the patient, which contained the same issues as the initial questionnaire with rates from 0 to 10; and another assessing the safety of the procedure, focusing on the description of adverse effects.
A new ultrasound skin examination was performed in predetermined areas of the face, in addition to new frontal and profile photographs, 30 days after the last application.
The photographs were analyzed and compared by a physician who did not participate in the study, but who also answered the questionnaire previously given to the physician who applied the product. The ultrasounds were compared in terms of dermal thickness and density.
The analysis of the results of each patient considered:
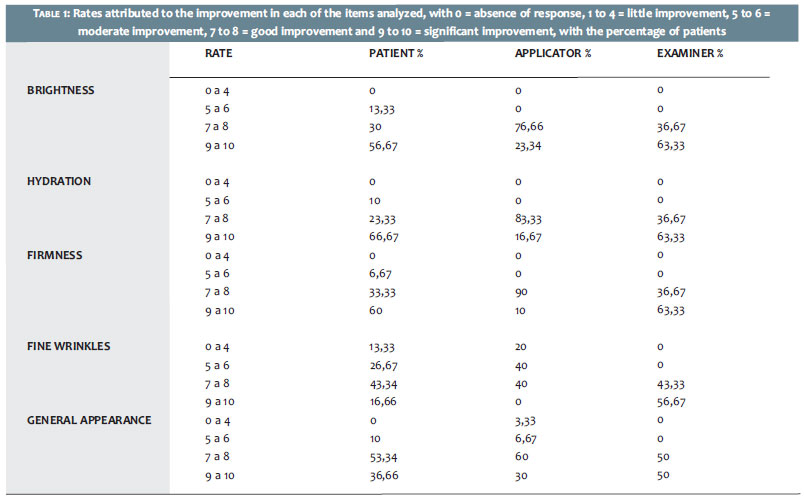
- The evaluation of individual patients with rates from 0 to 10 for the items: brightness, hydration, firmness, fine wrinkles, and overall appearance;
- The participating physician rates for those items;
- The external investigator physician's rates for those items;
- The results from the sonographic measurements of various facial points.
The rates for final results assessing the improvement in each of the evaluated items, attributed by the patients and participating and observing physicians 30 days after the last application, are shown in Table 1.
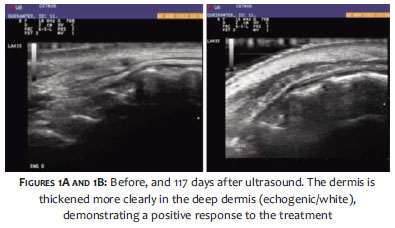
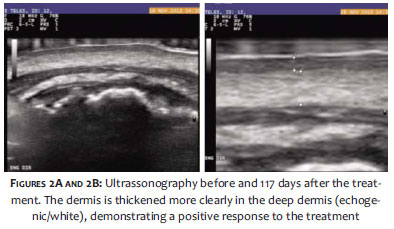
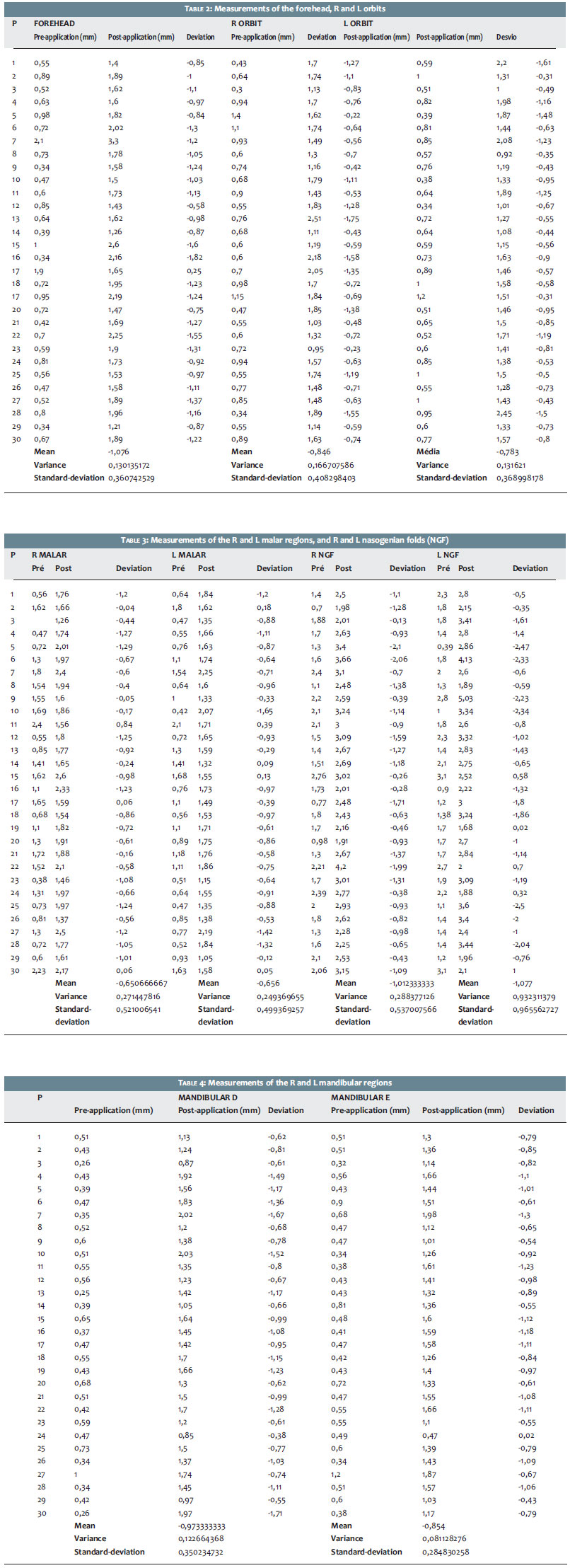
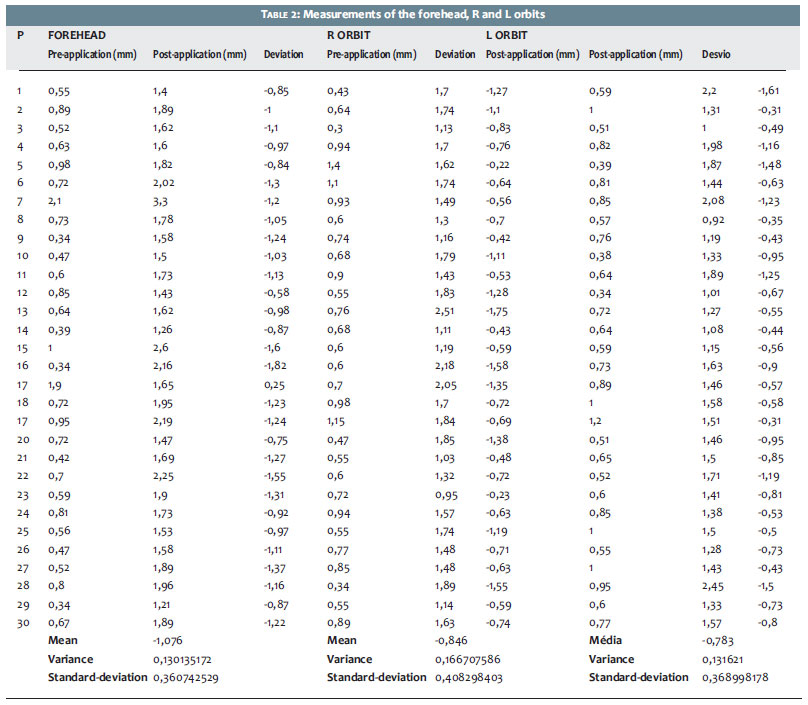
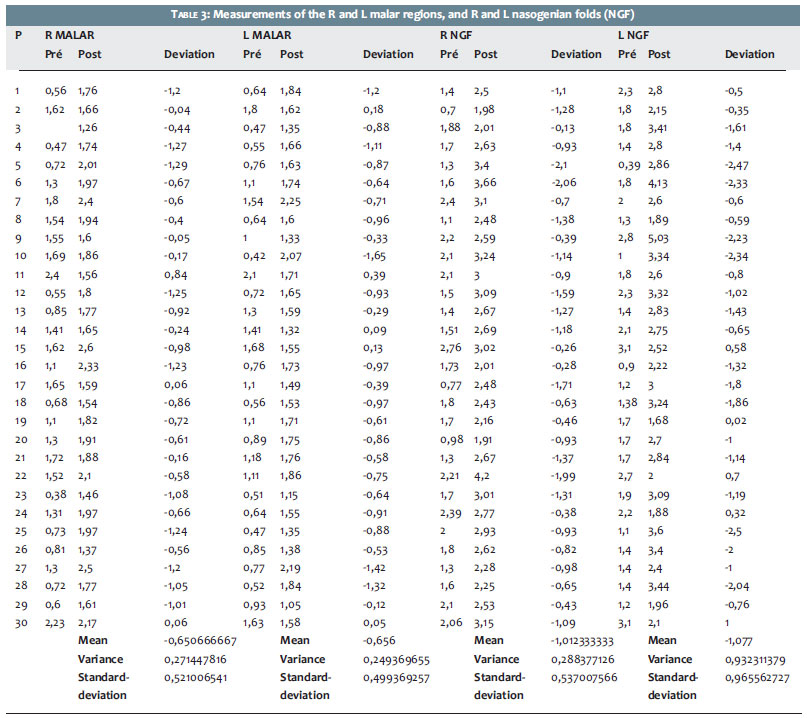
Regarding dermal thickness, measurements were carried out using 30MHz ultrasound in several areas of the face before and 117 days after the first application. The measurements are exemplified in Figures 1A and 1B and in Figures 2A and 2B, where the superficial dermis is hypoechogenic (gray) and the deep dermis is echogenic (white). The measurements were analyzed separately in their respective areas, as shown in Tables 2 to 4.
In the statistical analysis the paired t-test was applied, with the measurement of the skin's thickness being taken before and after 2 applications of the medicament. The following parameters were used:
- H0 or null hypothesis: states that there is no difference between the thickness before and after application;
- H1: implies significant alteration between the time before and after the applications.
The test used a normal, two-tailed model for the distribution of values, with alpha = 0.05%. In light of the values and determining a strength of 80%, the sample size of 30 patients was considered sufficient. Tables 1, 2, and 3 show the measurements of the dermis in the skin ultrasonography before and 15 days after the last application, with their respective standard deviations. The measurements were performed on the forehead, R and L periorbital regions, R and L malar regions, R and L nasogenian folds (NGF), and R and L mandibular regions.
The results of the statistical analysis of the measurements obtained through skin ultrasonography demonstrated that all areas studied showed significant differences after the application, concluding that within the three month period the application of the medicament through intradermotherapy has modified the skin's thickness.
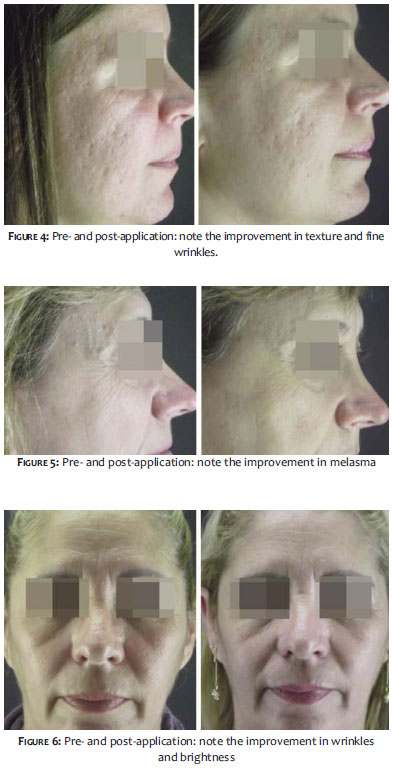
Therefore, the observations of the patients, participating lead physician, and blinded observer physician implied rates that ranged from 7 to 10, indicating answers from good to excellent (Figures 3 to 6).
Clinical signs of cutaneous aging are the result of alterations that the skin undergoes under the influence of UV radiation, the environment (such as pollution), eating and personal habits, and life style (such as smoking and stress, hormone levels and genetics). The loss of brightness and presence of sagging, and dryness in addition to the appearance of fine wrinkles, are the first signs of aging, leading many patients to seek treatment. In these cases, improvement in hydration and intake of nutrients often become the most effective measures, yielding long-lasting results.
Despite the fact that treatment with intradermotherapy has been used in France for more than 30 years, its results are still being questioned due to the lack of comparative studies with data taken both before and after the application to prove its efficacy. Several authors question the clinical improvement resulting from this treatment.24
The present study was aimed at analyzing and confirming whether or not the benefits of skin rejuvenation treatment with a combination of antioxidants, vitamin complexes, amino acids, coenzymes and noncross-linked hyaluronic acid can be confirmed, based on the opinion of the patients and the physician who applied the product, taking into considerationthe parameters of brightness, hydration, texture, and overall appearance of the skin of patients with mild to moderate clinical signs of photoaging. The analysis of photographs carried out before, during, and after the treatment also reinforces the critical analysis, which the study is intended to perform.
Ultrasonography of the skin with the 18MHz transducer proved an excellent way of assessing epidermal and dermal thickness, as seen in the photographs, due to its high resolution. This also facilitated the carrying out of studies aimed at analyzing the skin's thickness, since skin biopsies have always been very difficult to implement, for the patients are often not willing to undergo tests that leave scars.
In most patients, the ultrasound study demonstrated increased dermal thickness and dermal rearrangement, with the reorganization of fibers, which explains the improvement in skin texture, fine wrinkles, and acne scars, as observed in one of the patients.
The statistical analysis has shown that 30 patients (n = 30) is a suitable sample to assess the effectiveness of the treatment and the analysis of sonographic measurements in the periods before and after the treatment; it has also shown that there has indeed been improvement in dermal thickness with intradermal injections of the compound in association with antioxidants, vitamin complexes, amino acids, coenzymes, and noncross-linked hyaluronic acid.
The mean values of the scores assigned in the questionnaires by the patients, the physician who applied the product, and the blinded examiner physician have shown that most patients treated with superficial and deep intradermal injections (intradermotherapy) of the compound were very satisfied with the treatment. A fact that attracted attention was that several patients with melasma reported improvement with the treatment.
Regarding the safety, the analysis has shown that there was no occurrence of major side effects other than the formation of small hematomas that resolved quickly. Pain during application did not constitute an obstacle to the execution of the treatment.
As with any other technique, it is important to analyze the benefits, safety, efficacy, and standardization of intradermotherapy regarding its indication as a treatment. A proper selection of patients seems critical to its outcome. Its best indication seems to be related to patients with early signs of photodamage and who have mild to moderate skin dehydration, in addition to formation of fine wrinkles. The authors suggest that further studies be conducted to evaluate the efficacy of the studied technique in the treatment of melasma.
In thepresent study it was possible to observe that the intake of antioxidants (vitamins C, E, and glutathione), tissue nutrients in the form of vitamins (C, E, and B complex), coenzymes, nucleic acids, amino acids and hyaluronic acid without crosslinking, proved to be considerably effective for the improvement of dermal thickness and the reorganization of fibers, culminating with the improvement of mild to moderate signs of photodamage.
The authors would like to thank Rejuvene Medical for technical support in carrying out the present study.
1. Debacq-Chainiaux F, Leduc C, Verbeke A, Toussaint O. UV, stress and aging. Dermatoendocrinol. 2012;4(3):236-40.
2. Callaghan TM, Wilhelm KP. A review of ageing and an examination of clinical methods in the assessment of ageing skin. Part I: cellular and molecular perspectives of skin ageing. Int J Cosmect Sci. 2008;30(5):313-22.
3. Escoffier C, de Rigal F, Rochefort A, Vasselet R, Leveque JL, Agache PG. Age-related mechanical properties of human skin: na vivo study. J Invest Dermatol 1989;93(3):353-7.
4. Bottai G, Mancina R, Muraton M, DiGennaro P, Lotti T. 17 beta-estradiol proptects human skin fibroblastos and keratinocytes against oxidative damage. J Eur Acad Dermatol Venereol. 2013;27(10):1236-43.
5. Chang KC, Wang Y, Oh IG, Jenkins G, Freedman LP, Thompson CC, Chung JH, Nagpal S. Estrogen receptor beta is a novel therapeutic target for photoaging. Mol Pharmacol. 2010;77(5):744-50.
6. Draelos ZD. Nutrition and enhancing youthful-appearing skin. Clin Dermatol. 2010;28(4):400-8.
7. Proksch E, Jensen JM. Skin as an organ of protection. In: Wolf K, Goldsmith LA, Katz SI, Gilcherest BA, Paller AS, Leffell DJ, editors. Fitzpatrick,s Dermatology in General Medicine. 7th ed. New YorK:MacGrawHil Medical; 2010. p. 383-95.
8. Widgerow AD, Grekin SK. Effecting skin renewal: a multifaceted approach. J Cosmet Dermatol. 2011;10(2):126-30.
9. Bonté F. Skin moisturization mechanisms: new data. Annales Pharmaceutiques Françaises. 2011;69(3):135-41.
10. Verdier-Sévrain S, Bonté F. Hydration: a review on its molecular mechanisms. J Cosmet Dermatol. 2007;6(2):75-82.
11. Mammucari M. Mesotherapy, definition, rational and clinical role: a consensus report from the Italian Society of Mesotherapy. Eur Rev Med Pharmacol Sci. 2011;15(6):682-94.
12. Passi S, De Pità O, Grandinetti M, Simotti C, Littarru GP. The combined use of oral and topical lipophilic antioxidants increases their levels both in sebum and stratum corneum. Biofactors 2003;18(1-4):289-97.
13. Medydani M. Vitam E. Lancet. 1995;345(8943):170-5.
14. Passi S, De Pità O, Grandinetti M, Simotti C, Littarru GP. The combined use of oral and topical lipophilic antioxidants increases their levels both in sebum and stratum corneum. Biofactors. 2003;18(1-4):289-97.
15. Brown KL, Phillips TJ. Nutrition and wound healing. Clin Dermatol. 2010;28(4):432-39.
16. Ruiz K. Nutracêuticos na prática - terapias baseadas em evidências. São Paulo: Innedita; 2012.
17. Chan AC. Partners in defense: vitamin E and vitamin C. Can J Physiol Pharmacol. 1993;71(9):725-31.
18. Heinrich U, Tronnier H, Stahl W, Béjot M, Maurette JM. Antioxidant supplements improve parameters related to skin struture in humans. Skin Pharmacol Physiol. 2006;19(4):224-31
19. Chan AC. Partners in defense: vitamin E and vitamin C. Can J Physiol Pharmacol. 1993;71(9):725-31.
20. Azuma K, Ouchi Y, Inoue S. Vitamin K: novel molecular mechanisms of action and its roles in osteoporosis. Geriatr Gerontol Int. 2013 Mar 26. [Epub ahead of print].
21. Jurkic LM, Cepanec I, Pavelic SK, Pavelic K. Biological and therapeutic effects of ortho-silicic acid and some ortho-silicic acid releasing compounds: new perspectives for therapy. Nutr Metab (Lond). 2013;10(1):2.
22. Choi HR, Kang YA, Na JI, Hush CH, Kim KH, Park KC. Oligosaccharides of hyaluronic acid increased epidermal cell stemness by modulation of integrin expression. J Cosmet Dermatol. 2012;11(4):290-6.
23. Papakonstantinou E, Roth M, Karakiulakis G. Hyaluronic acid: a key molecule in skin aging. Dermatoendocrinol. 2012 Jul;4(3):253-8.
24. El-Domyati M, El-Ammawi TS, Moawad O, El-Fakahany H, Medhat W, Mahoney MG, et al. Efficacy of mesotherapy in facial rejuvenation: a histological and immunohistochemical evaluation. Int J Dermatol. 2012;51(8):913-19.
Study performed at the Cosmetic Dermatology Ambulatory of the Dermatology Discipline of the Faculdade de Medicina do ABC (FMABC)-Santo André (SP), Brazil.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}