


Cristiane Lüdtke1; Daniela Moraes Souza1; Magda Blessmann Weber2; Aline Ascoli3; Fernanda Swarowski3; Cíntia Pessin4
Keywords: EYES; QUALITY OF LIFE; DERMATOLOGY.
Periorbital hyperchromia, peripalpebral hyperchromia, dark eyelids, dark eye circles or simply "dark circles", despite being a mere difference in color between the palpebral skin and the rest of the facial skin, can have a major impact on the quality of life by causing an appearance of fatigue and premature aging.1-4 There are two types of dark circles: vascular and melanic, nevertheless it is believed that most have mixed components, with melanin and hemosiderin being found in almost all types of dark circles, to a greater or lesser degree.2
Vascular dark circles, the predominant type, have an autosomal dominant inheritance pattern. They usually appear earlier in life, during childhood or adolescence. They are more common in ethnic groups that include people of Arabic, Turkic, Indian, or Iberian backgrounds. The diagnosis of this type of dark circles is carried out by applying traction to the lower eyelid, making it more transparent and therefore easier to view the vessels underneath the skin.2-4 In this type of periorbital hyperchromia there is no change in the color of the skin, however the eyelid has a darker hue due to the visible presence of dilated vessels. It is believed that cutaneous hyperchromia occurs due to the deposition of hemosiderin when there is dermal blood extravasation.2 Smoking, consumption of alcohol, mouth breathing, sleep deprivation, the use of vasodilator drugs, prostaglandin analogues based eye drops, contraceptives, chemotherapy and antipsychotics are factors that can contribute to this process through the stasis of blood vessels, leading to a change of color in the area. Moreover, the presence of conditions that involves the retention of water and eyelid edema (thyroid, kidney, heart, and lung diseases) cause a worsening of the unaesthetic appearance of dark circles. The ideal treatment should include the discontinuation of possibly identified triggering factors, the removal of preformed hemosiderin, and photoprotection.2-4
The predominantly melanic periorbital hyperchromia typically affects older people with higher skin types, however it can also occur in patients with lower skin types (also usually elderly) as a result of excessive and cumulative exposure to the sun.3
In the literature, there is little dissemination of epidemiological data and factors associated with periorbital hyperchromia. The present study is aimed at evaluating those variables in patients with dark circles.
To assess the prevalence of periorbital hyperchromia and possible pathogenetic factors in a population sample of a public dermatology service of a university in southern Brazil.
A prospective cross-sectional study was conducted at the public dermatology service of the Universidade Federal de Ciências da Saúde de Porto Alegre (RS), Brazil. The study was approved by the research ethics committee of the institution where the study was conducted.
Patients who attended medical appointments at the service from November 2011 to April 2012 with complaints of dark circles were invited to participate. All were clarified by the interviewer as to the purpose of the study and about the protection of their privacy, ensuring their anonymity would be preserved in the presentation of the study's results. A term of free and informed consent was signed by all participants, who were then administered a questionnaire by the researchers in order to collect data.
The inclusion criteria for the study were: patients who attended the dermatology service, of both genders and all races, over 18-years-old, and who had signed the free and informed consent term, and agreed to participate in the study. Patients who did not agree to participate, did not sign the term of consent and were under 18-years-old were excluded.
Data collected included: age, gender, skin phototype, age of onset of dark circles, use of sunscreen and corrective makeup, previous treatments for dark circles, habit of snoring, presence of deviated septum, atopic dermatitis, asthma, rhinitis, comorbidities, use of mouth breathing device and continuous medications, in addition to the presence of dark circles in the family and number of hours of sleep per day.
The data were tabulated in an Excel database and distributed using the Kolmogorov-Smirnov test.
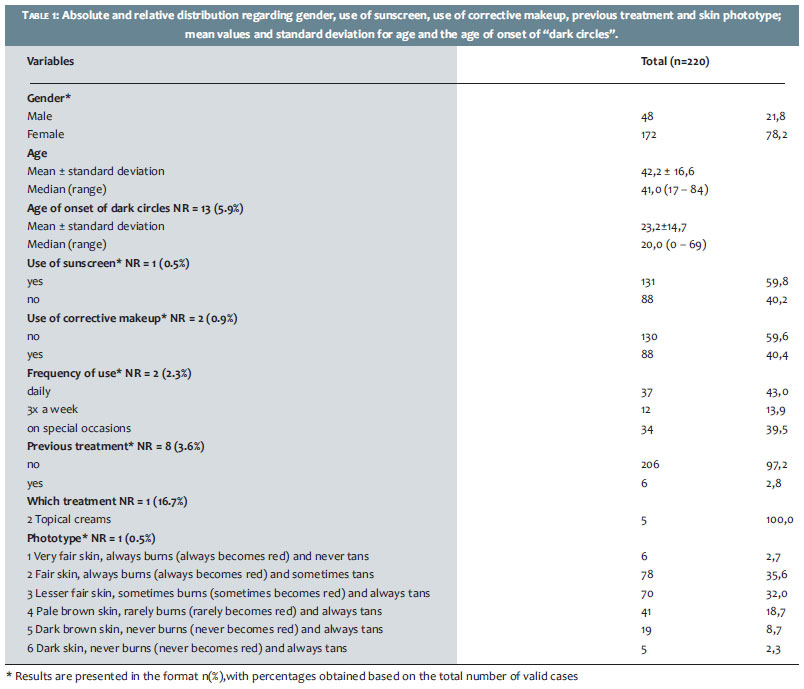
During the study, 220 patients were investigated. Of these, 78.2% (n = 172) were women. The mean age was 42.2 years (SD = ± 16.6 years), with a minimum of 18 and a maximum 84 years.
Regarding the age of onset of dark circles, the mean value was 23.2 years (SD ± 14.7 years). Regarding the phototype, the sample studied had greater participation of phototypes II (35.6%, n = 78) and III (32.0%, n = 70).
The use of sunscreen was reported by 59.8% (n = 131) of patients. Regarding the use of corrective makeup to camouflage dark circles, 40.4% (n = 88) of respondents reported its use, with most reporting daily use (43.0%, n = 37).
When asked whether they had undergone previous treatment, a small portion of the sample answered positively (2.8%, n = 6), informing that only topical cosmeceuticals had been used previously (Table 1).
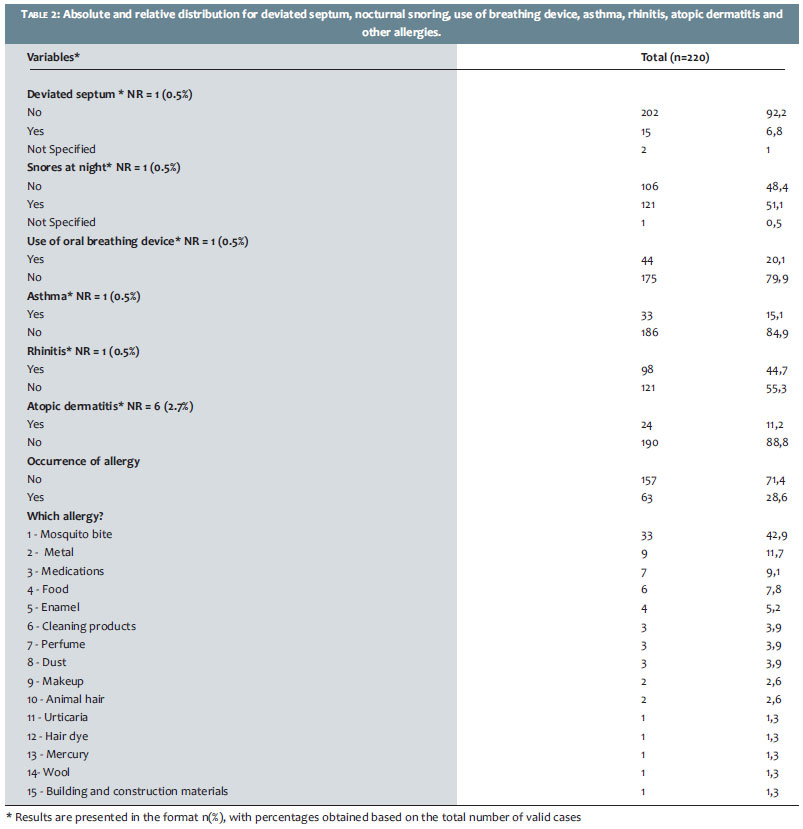
Occurrence of deviated septum was observed in 6.8% (n = 15), nocturnal snoring in 48.4% (n = 106), asthma in 15.1% (n = 33), rhinitis in 44.7% (n = 98), and atopic dermatitis in 11.2% (n = 24).
Mouth breathing was reported by 20.1% (n = 44) of the investigated patients. Regarding the presence of some other type of allergy, 28.6% (n = 63) answered positively, with the most cited being mosquito bites (42.9%, n = 33) (Table 2).
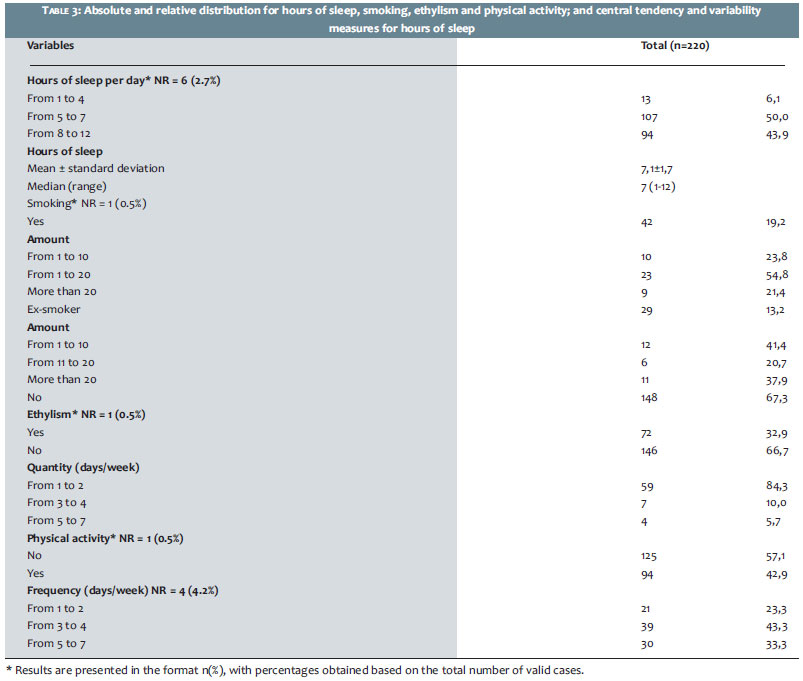
Regarding hours of sleep, half of the sample (n = 107) reported sleeping 5 to 7 hours per day, with an average of roughly 7 hours per day (SD = 1.7 hours/day), a minimum of 1 and maximum of 12 hours per day.
Smoking habits were reported by 19.2% (n = 42) of the investigated patients, of which 54.8% (n = 23) reported smoking 11 to 20 cigarettes daily (median = 20 cigarettes/day). It was also verified that 13.2% (n = 29) of the patients being investigated were ex-smokers.
As for drinking habits (ethylism), 32.9% (n = 72) of respondents reported drinking alcohol once or twice a week (84.3%, n = 59).
Practicing some physical activity was reported by 42.9% (n = 94) of the respondents, with 43.3% (n = 39) carrying it out three or four times a week (Table 3).
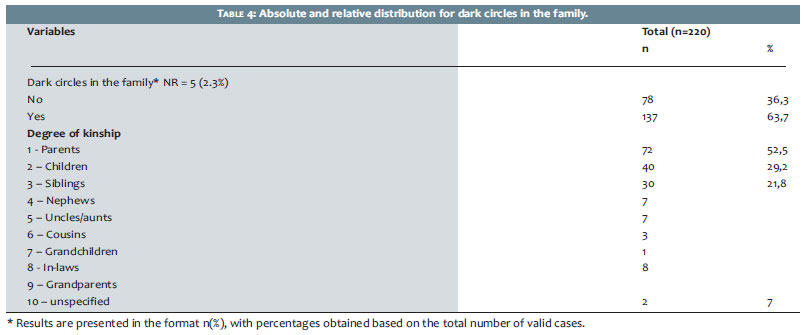
Regarding the presence of dark circles in the family, 63.7% (n = 137) of patients responded affirmatively. As for the degree of kinship, the most frequently cited were parents (52.5%, n = 72), children (29.2%, n = 40), and siblings (21.8%, n = 30) (Table 4).
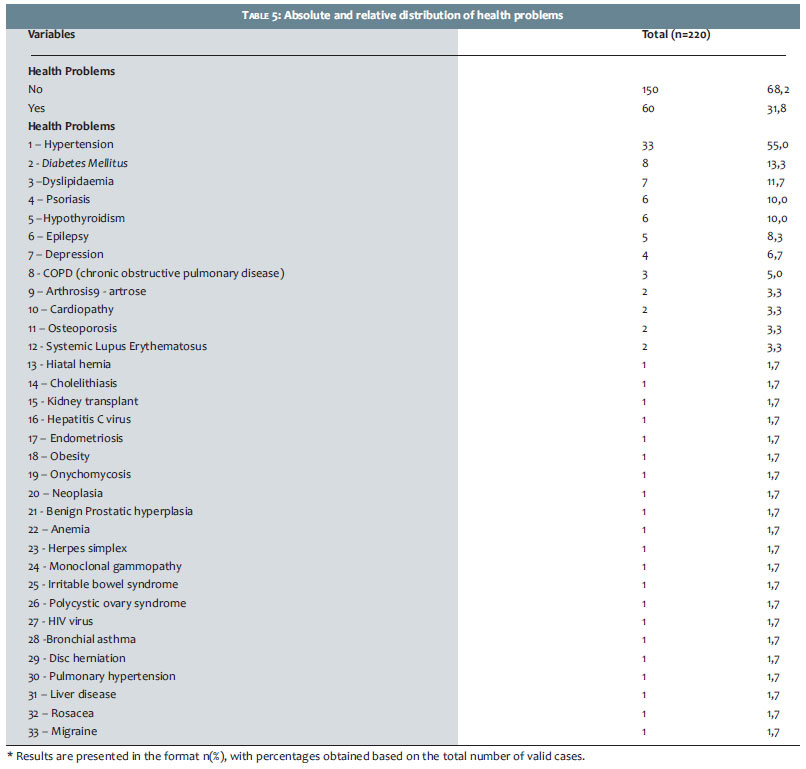
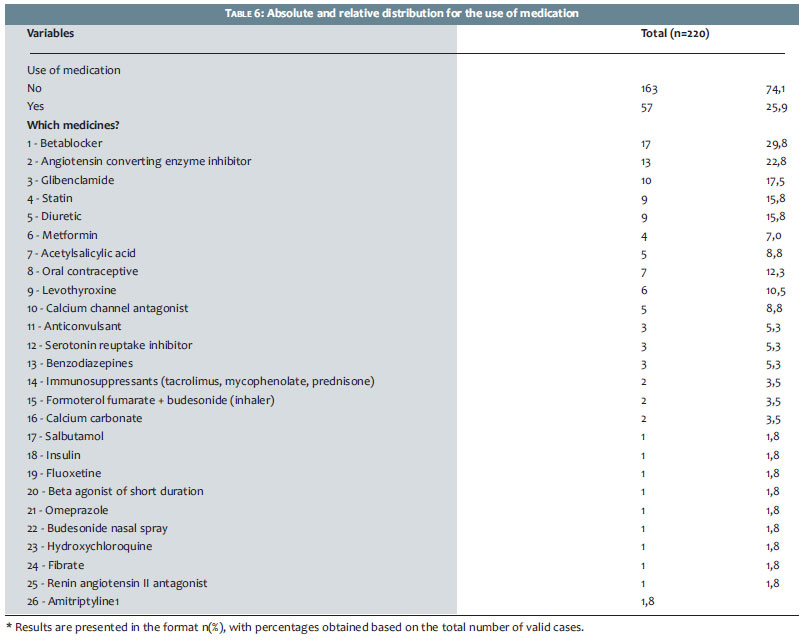
The presence of comorbidities was seen in 31.8% of the sample, with the most frequent being arterial systemic hypertension (55%), diabetes mellitus (13.3%) and dyslipidemia (11.7%) (Table 5). The continuous use of medications was reported by 25.9% of respondents, with the most frequently cited being beta-blockers (29.8%) and the angiotensin converting enzyme inhibitor (22.8%) (Table 6).
Periorbital hyperchromia, also called dark circles, is more often observed in women-particularly in brunettes-being caused by physiological and genetic factors.1
In the present study-and in line with the literature-the majority of patients were female. Regarding phototypes, the study group had a concentration of types II and III, a fact that differs from many studies. These results may be due to the population studied, primarily Caucasian, as demonstrated by the prevalence of skin phototypes II and III.
Regarding the age, periorbital hyperchromia can start in childhood or in adulthood. In the first case, it usually has a pattern of family heritage, being mostly vascular. In the second case, it is mostly melanic.2 Most dark circles, however, have mixed components.2 In the present study, most patients were adults who experienced the onset of periorbital hyperchromia in late adolescence. In those cases, it was impossible to determine whether the onset was related to melanic or vascular predominance, because the patients were not classified by their type of dark circles. However, the majority had a family history, which favors the vascular component. As for the use of sunscreen, it is known that the product acts in preventing dark circles.5 In the present study, daily use of sunscreen was relatively frequent, probably due to the intention of the patients to better control the condition.
Conditions such as smoking, physical inactivity, ethylism, deviated septum, asthma, rhinitis, atopic dermatitis and other allergies, mouth breathing and sleep deprivation can contribute to palpebral hyperchromia due to the stasis of blood vessels.2,6 In the present study, those factors were found in a considerable part of the sample, further strengthening their correlation with the presence of dark circles. Regarding the presence of diseases most frequently associated with periorbital hyperchromia (thyroid, kidney, heart, and lung diseases), they were rarely reported by the studied patients. In the present study, the most frequently mentioned comorbidities were arterial systemic hypertension, diabetes mellitus, and dyslipidemia-conditions that can develop into some of the already mentioned diseases. The use of vasodilators, prostaglandin analogues eye drops, chemotherapeutic agents, contraceptives and antipsychotics, all of which, according to the literature, usually contribute to periorbital hyperchromia, have also been rarely reported in the studied sample.2,3 The medications more frequently informed were beta-blockers and angiotensin converting enzyme inhibitors, probably due to the predominance of cases of hypertension in the studied population.
In the present study, periorbital hyperchromia was more frequently observed in women in their 40's, with low skin phototypes, who reported daily use of sunscreen, sedentary habits, sleep deprivation, and family history of dark circles. Despite this epidemiological profile being similar to that described in the literature, further studies are necessary in order to allow dermatologists to develop better management strategies for this condition, thereby contributing to improvements in the patients' self-esteem and quality of life.
1. Sampaio S, Rivitti E. Dermatologia 2ª ed. São Paulo: Artes Médicas; 2000.
2. Costa A, Basile DVA, Medeiros VLS, Moisés AT, Ota SF, Palandi JAC . Peeling de gel de ácido tioglicólico 10% opção segura e eficiente na pigmentação infraorbicular constitucional. Surg Cosmet Dermatol.2010;2(1):29-33.
3. Steiner D. Clínica Denise Steiner [Internet]. Acessado em [06 Jun 2013].Disponível em: http://www.denisesteiner.com.br/derma_estetica/olheiras2.htm.
4. Freitag FM, Cestari TF. What causes dark circles under the eyes? J Cosmet Dermatol. 2007;6(3):211-5.
5. Oshima H, Takiwaki H. Evaluation of dark circles of the lower eyelid: comparison between reflectance meters and image processing and involvement of dermal. Skin Res Technol. 2008;14(2):135-41.
6. Kede MPV, Sabatovich O. Dermatologia Estética. São Paulo: Editora Atheneu; 2004. p.259.
Study conducted at the Universidade Federal de Ciências da Saúde de Porto Alegre (UFCSPA)-Porto Alegre (RS), Brazil.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}