


Paula Luz Stocco1; Guilherme Fonseca2; Lucas Emanuel de Lima Azevedo1; Thais Bittencourt Gonçalves Teles1; Carmélia Matos Santiago Reis3
The reconstruction of defects resulting from tumor resection is a challenge for the surgeon, who should get good results both functional and aesthetic. The objective of the present study is to describe the surgical technique used in a 78-year-old male patient with the diagnosis of squamous cell carcinoma in the lower lip and who underwent excision of the lesion and reconstruction with the Karapandzic technique. This flap is employed in the reconstruction of surgical defects that cover 40-75% of the lip's extension.
Keywords: CARCINOMA, SQUAMOUS CELL, SURGICAL FLAPS, LIP NEOPLASMS.
Squamous cell carcinoma is the most common malignant neoplasm of the lips. It is an aggressive and invasive tumor, which can metastasize if not treated early and radically. Only 5% of the neoplasms of the lip occur in the upper lip, and the vast majority are basal cell carcinomas. The other 95% affect the lower lip, where the squamous cell carcinoma is predominant due to greater exposure to ultraviolet radiation. This anatomical area is of great interest due to the high frequency of the condition, which involves the buccal cavity's natural sphincter.1-6
The reconstruction of defects resulting from tumor exeresis poses a challenge to the surgeon, who must aim for good functional and aesthetic results. For that reason, numerous techniques are described for the reconstruction of this anatomic region.1-6
The following techniques are available among surgical procedures for the treatment of lesions in the lower lip: shaving, "V"excision, with or without the leveling of the vermilion; Karapandzic flap; Estlander flap; and reconstruction with Bernard-Burrow-Webster flap.1-6
The shave or leveling technique is used in cases of superficial lesions affecting the mucosa and submucosa, but which do not infiltrate the musculature. The "V" technique excision , with or without leveling of the vermilion, is indicated for cases where a large lesion covers a part of the vermilion, requiring that it be excised in a wedge shape. Resections of up to 30% of the lip allow for a primary suture without tension. Resections leading to defects of between 30-40% are best addressed through resections in "W" or using labial flaps.1-6
The Karapandzic technique is suitable for repairing central defects of the lower lip through rotation and advancement of up to ¾ of the lip, preserving the sphincter function, innervation, and irrigation. The Estlander technique (pedicled lip transfer flap) is used when 30% of the lip must be ressected and may be substituted with a flap made from the upper lip. That flap's maximum length must be greater than 1.5 cm or 2.0 cm, which corresponds to about ¼ of the length of the lip. The reconstruction technique using a Bernard-Burrow-Webster flap is preferable for use with defects of up to 65%, when the ressection results in a major defect that needs to be reconstructed with vascularized flaps.1-6
The Karapandzic and Bernard-Burrow-Webster flaps are among the more frequently used options for reconstructing large lip defects. The Karapandzic flap is suitable for defects covering 2/3 of the length of the lower lip. In cases of larger defects the resulting microstomia contraindicates this procedure. In total or subtotal labial defects, the Bernard-Burrow-Webster flap remains a good reconstructive option.1-6
The factors influencing the selection of the treatment type and technique to be employed are related to the tumor and patient.1-6
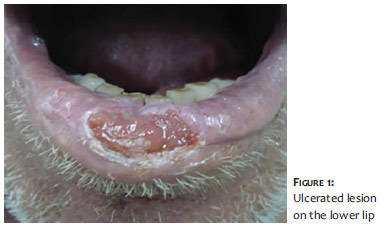
The case involves a seventy-eight-year-old male patient with an ulcerated lesion in the lower lip that had developed for six months, with progressive growth (Figure 1) and absence of regional lymphadenopathy on palpation. The clinical diagnosis of squamous cell carcinoma was confirmed through biopsy.
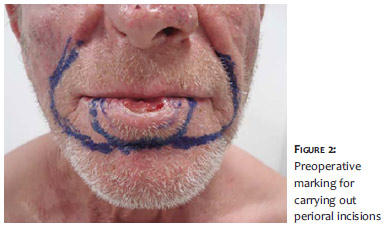
Under ambulatorial regimen and local anesthesia, the patient underwent an uneventful excision of the lesion and reconstruction with the Karapandzic myocutaneous flap technique. The preparation of the flaps consisted of bilateral perioral incisions, originating in the lower borders of the surgical defect and extended along the mentolabial and nasolabial grooves (Figure 2).
The orbicularis oris muscle and oral mucosa were incised up until the point of the labial commissures. A delicate dissection of planes was carried out so that the incisions did not reach the oral mucosa laterally. Advanced myocutaneous flaps were then prepared to cover the defect. The neurovascular structures were spared, thus preserving the lip's sensitivity and motility (Figures 3 and 4).
The flaps were medially oriented, with the suturing of the mucosa, orbicularis oris muscle, and skin in three successive planes, allowing the restoration of the oral sphincter's continence (Figure 5).
The aesthetic and functional result was satisfactory, given that the sutures conincided with the natural grooves. The oral continence, the sensitivity, and mobility of the lip were preserved. Nevertheless, there was a slight microstomia with no functional impact that can be mitigated with commissurotomy (Figure 6).
One year after the procedure, the patient had no signs of local recurrence or local-regional metastasis.
The flap described by Karapandzic in 1974 is one of the options for reconstruction of large defects of the lip. It is based on the anatomical preservation of the facial nerve's vascular pedicles, which maintain the lip's future irrigation and functionality, with the advantage of being carried out in a single surgical event and possibly under local-regional anesthesia. 1-5 It is the appropriate flap to correct defects affecting 40-75% of the length of the lower lip, and can be applied in reverse in the reconstruction of the upper lip. The Karapandzic flap has as its main virtue the preservation of the mobility of the lower lip and its sensitivity, as well as the oral continence. Its greatest drawback is microstomia, which also occurs-to a greater or lesser degree-with other flap techniques used in the reconstruction of full thickness surgical defects. 1-6
1. Brinca A, Andrade P, Vieira R, Figueiredo A. Retalho de Karapandzic e retalho de Bernard-Burrow-Webster na reconstrução do lábio inferior. An Bras Dermatol. 2011;86(4 Supl 1):S156-9.
2. Fonseca M, Garcia G. Reconstruccion de labio con Técnica de Karapandzic. Cir Plas Iberolatinoam. 2007;33(1):57-62.
3. Sbalchiero JC, Anlicoara R, Cammarota MC, Leal PRA. Reconstrução labial: abordagem funcional e estética após ressecção tumoral. Rev Soc Bras Cir Plast. 2005;20(1):40-5.
4. Faveret P, Franco D, Boghossian LC, Medeiros J, Franco T. Carcinoma de lábios: análise de tratamento cirúrgico realizado em hospital universitário. Rev Bras Cir Craniomaxilofac 2009;12(4):155-8.
5. Conti LA, Carvalho MM, Machado Filho CDS, Hayashida ME, Ferraz TS, Gonçalves Jr. BF. Reconstrução do lábio inferior com retalhos de Karapandzic e Gilles após excisão de carcinoma espinocelular. Surg Cosmet Dermatol. 2012;4(2):195-9.
6. Karapandzic M. Reconstrution of lip defects by local arterial flaps. Br J Plast Surg. 1974;27(1):93.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}