


Alex Panizza Jalkh1; Anne Caroline da Silva Menezes2; Alcidarta dos Reis Gadelha3
Syringocystadenoma papilliferum is a rare, benign tumor, most common in the scalp and face. It can present as an independent lesion or be associated with nevus sebaceous of Jadassohn. Rare cases of this tumor located in the thigh have been reported in the literature. The present article reports the case of a patient with syringocystadenoma papilliferum, distinguished by its intradermal tubular apocrine papillary component.
Keywords: ADENOMA, SWEAT GLAND; SKIN NEOPLASMS; NEOPLASMS, ADNEXAL AND SKIN APPENDAGE.
Syringocystadenoma papilliferum (SCAP) is an uncommon, benign adnexal tumor of the sweat glands. It is often located on the face, scalp, or neck, and can be present at birth, arise during childhood, or appear later on at an advanced age.1 Lesions are diverse and nonspecific, and can manifest, for instance, as a solitary plate or papules and multiple nodules, usually pinkish or winy with a verrucous erosive surface and a soft consistency.2
In most cases, the size of the SCAP increases during puberty and can be associated with other benign tumors, including the nevus sebaceous of Jadassohn, which is present in 40% of cases. Additionally, development of basal cell carcinoma (BCC)is reported in up to 10% of cases-which, in the majority of instances, presents in coexistence with nevus sebaceous.1
SCAP was first reported by Peterson in 1892 as a tumor of the sweat glands, and since Shiefferdecker differentiated sweat glands into apocrine and eccrine (in 1917), attempts to clarify the nature of the tumor are still controversial.3 Although eccrine origin has been observed in some tumors of this variety, a differentiation pattern that is predominantly apocrine is currently accepted as the norm.1
The present study is aimed at highlighting the SCAP's unusual location in this case, as a means of contributing to the differential diagnosis of atypical linear verrucous lesions in the thigh, and to the proper treatment of this rare disease.
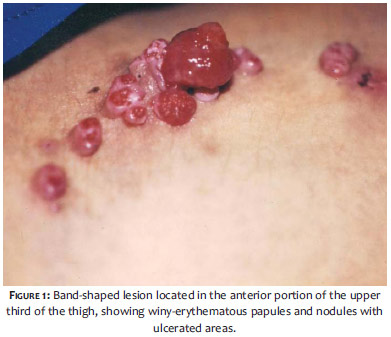
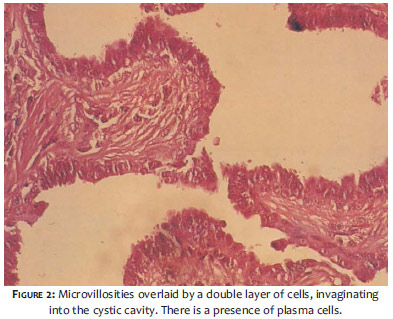
A 24-year-old, Caucasian, patient, born and residing in Manaus, the capital of the northern Brazilian State of Amazonas, alleged to having a lesion since birth that had increased in size, and started producing exudate and presenting pruritus after puberty. A band-shaped lesion, located in the upper third of the anterior side of the left thigh, measuring approximately 8 x 2cm was observed in the clinical examination. It was composed of exudative, prutritous, and not-painful-to-the-touch winy-erythematous papules and nodules, with a smooth surface and firm consistency (Figure 1). Histopathology revealed cystic invaginations protruding into the dermis (Figure 2). In the lumen, there were villosities overlaid by two layers of cells: the innermost, with columnar cells, showing secretion due to "decapitation"; and the outermost, with cuboidal cells. In the upper dermis, there was infiltrate that was rich in plasmocytes.
In 1917, Stokes called nevus syringadenomatus papilliferum a neoplasm located in the skin of the thigh of a female patient. 3 Since then, many cases have been published in the medical literature, mostly referring to those located on the head and neck (75%), and on the trunk (20%). In the present study, the SCAP had multiple linear lesions-similar to the eight cases reviewed by Rammeh-Rommani et al.2
More recently, two cases have described instances in which multiple tumors have arisen simultaneously, originating from sebaceous nevi.1 As with Stokes' initial case, the lesion in the patient described in the present study, was located on the thigh, tumors on the body's extremities being a less common occurrence. This patient's lesion was present at birth, as is the case in 51% of these tumors. The authors emphasize the unusually exuberant growth of the lesion, its dimensions being reported at 8 x 2cm.
This kind of tumor has been described as asymptomatic, although sometimes it presents pain and pruritus.7,8 As with other case reports, the patient in the present study had pruritus and discomfort due to the lesion's exudative and pruritic character, in addition to the obvious compromise of the aesthetic appearance. Present in 40% of cases, the association of SCAP with nevussebaceous 3 was not detected in the referred patient.
Due to the rare nature of the neoplasm, the authors highlight the importance of the histological examination to establish the differential diagnosis.1 The surgical excision of the lesion resulted in its cure.
The authors warn about the very rare possibility of cases of syringocystadenocarcinoma papilliferum arising from SCAP, which can be recognized due to a nuclear atypia and increased mitotic activity combined with an invasive character.10
1. Bruno CB, Cordeiro FN, Soares FES, Takano GHS, Mendes LST. Aspectos dermatoscópicos do siringocistoadenoma papilífero associado a nevo sebáceo. An Bras Dermatol. 2011;86(6):1213-6.
2. Rammeh-Rommani S, Fezaa B, Chelbi E, Kammoun MR, Ben Jilani SB, Zermani R. Syringocystadenoma papilliferum: report of 8 cases. Pathologica. 2006;98(2):178-80.
3. Stokes JH. A clinico-pathologic study of an unusual cutaneous neoplasm combining nevus syringadenomatosus papilliferus and a granuloma. J Cutan Dis. 1917;35:411-9.
4. AYK Chan, NM Luk, WYM Tang, WY Lam. Syringocystadenoma papilliferum presenting as linearly arranged erythematous papules over medial thigh. Hong Kong J Dermatol Venereol. 2006;14(2):143-5.
5. Malhotra P, Singh A, Ramesh V. Syringocystadenoma papilliferum on thigh:um unusual location. Indian J Dermatol Venereol Leprol. 2009;75(2):170-2.
6. Philipone E, Chen S. Unique case: Syringocystadenoma papilliferum Associated with an eccrine nevus. Am J Dermopathol. 2009;31(8):806-7.
7. Karg E, Koron I, Varga E, Ban G, Turi S. Congenital Syringocistadenoma papilliferum. Pediatr Dermatol. 2008;25(1):132-3.
8. Pinkus H. Life history of naevus syringadenomatosus papilliferus. Arch Dermatol Syphilol. 1954;69:305-322.
9. Patterson JW, Straka BF, Wick MR. Linear syringocystadenoma papilliferum of the thigh. J Am Acad Dermatol. 2001;45(1):139-41.
10. Yap FB, Lee BR, Baba R. Syringocystadenoma papilliferum in an unusual location beyond the head and neck region: a case report and review of literature. Dermatol Online J. 2010 Oct 15;16(10):4.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}