


Renata Heck1; Cristina Rossi2; Isabel Cristina Palma Kuhl3; Lucio Bakos4
Onychomycosis is a very common condition in Brazil and one whose current treatments yield low cure rates, potential adverse effects, and drug interactions that limit their use. Recent studies have demonstrated laser therapy as a new, safe, and effective treatment option. This treatment was performed in 12 patients (with a total of 20 affected nails), with 3 application sessions of 1,064nm long pulse Nd:YAG laser, in two-week intervals. The results corroborate the current data of good clinical response and safety.
Keywords: ONYCHOMYCOSIS, LASERS, ADVANCED TREATMENT.
Onychomycosis is a fungal infection of the nail bed or nail matrix. It is estimated that about 4-18% of the world population might be affected.1-3
The treatment of the condition involves the use of topical and systemic drugs. In recent studies, the use of 8% ciclopirox olamine enamel showed effective cure (mycological cure and <10% of the nail affected) of 6.5-12.0% and total cure (mycological cure and and <0% of the nail affected) of 5.5-8.5%.4 Systemic agents, such as itraconazole, terbinafine, and fluconazole are more effective in treating onychomycosis,5 however adverse effects and drug interactions limit their use. Cure rates of those drugs are respectively 59±5%, 76±3%, and 48±5%.6
Recent publications report laser therapy as a treatment option for onychomycosis,4,7 which can be of great therapeutic value due to its absence of potential for drug interactions and renal/hepatic toxicity.
The non-ablative 1,064 nm Nd:YAG long pulsed laser (Neodymium Yttrium Aluminum Garnet), whose chromophores are melanin, hemoglobin, and water, acts on the dermis, reaching a depth of up to 5mm.
A recent study has shown that the 1,064 nm Nd:YAG laser had a significant effect on T. rubrum, inhibiting the growth of colonies in vitro.8 The melanin present in the wall of the fungal cells acts as the chromophore, justifying the action of the laser. Another mechanism involved can be the action of short duration pulses that would lead to microcavitation and acoustic shock waves, resulting in the mechanical damage of the fungi.8
Other studies have demonstrated mycological cure rates of 87.5% after 2 or 3 sessions with 1,064 nm Nd:YAG laser in onychomycosis in the halluces,7 and clinical improvement in 79% of patients after a single session, without any severe adverse effects.4
Gupta et al. treated 71 patients (128 nails) with a single laser session and observed a statistically significant improvement in 65.0% of them after six months.4
After approval by the Ethics Committee, the authors conducted a prospective, open, uncontrolled study, which included the first 12 patients who met the inclusion criteria, who did not present any exclusion criterion and had agreed to take part in the assessment.
Inclusion criteria were: patients from the Dermatology Service's Ambulatory Clinic of the Hospital de Clínicas de Porto Alegre (HCPA) and from the Universidade
Federal do Rio Grande do Sul (UFRGS) Porto Alegre (RS), Brazil - diagnosed with onychomicosis of halluces, confirmed by direct mycological examination and/or culture compatible with dermatophyte infection, and who were capable of reading, understanding, and signing the Term of Informed Consent (TIC).
Exclusion criteria were: use of systemic antifungal drugs in the previous 6 months, alteration in the nail pigmentation due to topical therapy, presence of subungual hematoma or nevi, bacterial infection, or nail diseases concomitant to pregnancy.
Selected patients signed the TIC and underwent pretreatment photographic documentation (Sony® DSC H20). An evaluation of pre-existent comorbidities and treatments was carried out. 1,064 nm Nd:YAG laser (platform Etherea,® Industra Technologies Br) was applied, spot size = 6 mm , pulse duration= 40 ms, fluence = 50-80 J/cm2, in crossed passes (horizontal passes followed by vertical passes), 2 passed with 1 minute intervals between them, covering the entire surface of the nail using the technique described by Hochman.7 All patients underwent 3 sessions at biweekly intervals. Adverse effects were recorded during application and on the following day through a telephone call, rating the pain symptoms as mild, moderate, or severe.
Ninety days after the last session, the patients underwent a final clinical evaluation and photographic documentation. Images were recorded following the same regimen and photographic techniques used previously.
The evaluation of results was carried out by analyzing pre-treatment photographs and comparing them to the final images. The images were magnified to better assess and subjectively quantify the percentage of improvement. New, direct mycological examination and culture were carried out after the third session.
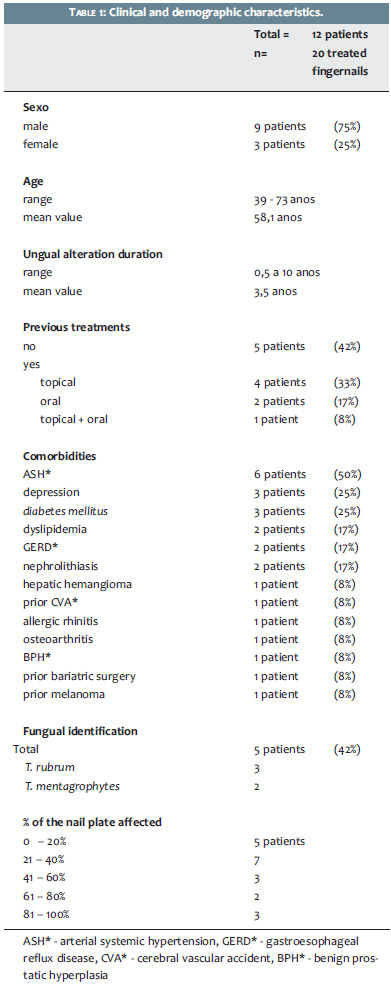
The 12 patients (9 women and 3 men, 75% and 25% respectively, age range between 39 and 73 years with a mean value of 58 years) received treatment in 20 affected nails. The timing of the ungual alterations varied from 6 months to 10 years, with a mean value of 3.5 years. Of all patients, 7 (58%) had already undergone previous treatments: 2 (17%) oral treatments, 4 (33%) topical treatments, and 1 (8%) topical and oral treatments. Eleven patients (92%) had comorbidities, the most common being: hypertension, depression, and diabetes mellitus, with only one smoker. The fungal agent was identified through culture in only 5 cases (2 Trichophyton mentagrophytes and 3 Trichophyton rubrum). As for the affected area, 5 patients had up to 20% of the nail plate affected, 7 patients had 21-40%, 3 patients had 41-60%, 2 had 61-80% and 3 patients had 80-100%. (Table 1)
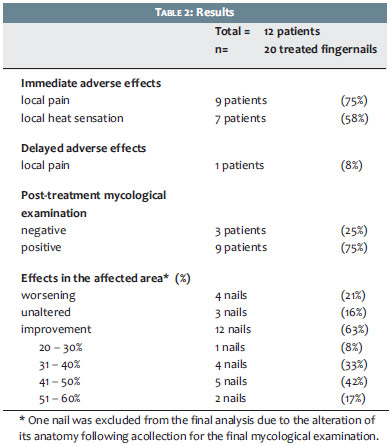
The immediate adverse effects included local pain (mostly described as a mild burning sensation reported by 9 of 12 patients (75%)) and local heat (reported by 7 patients (58%)). Only one patient (8%) had a delayed adverse effect, reported as mild local pain, which subsided after 24 hours.
All patients included in the study completed the evaluation. The mycological examination collected 3 months after the last session was negative in 3 patients (25%). In the other 9 patients, the samples remained positive, with the causative agent being identified in 3 cases.
The affected area 3 months after the last session was calculated based on the analysis of the photographs. One nail was excluded from the analysis for having been cut during the collection of mycological examination.
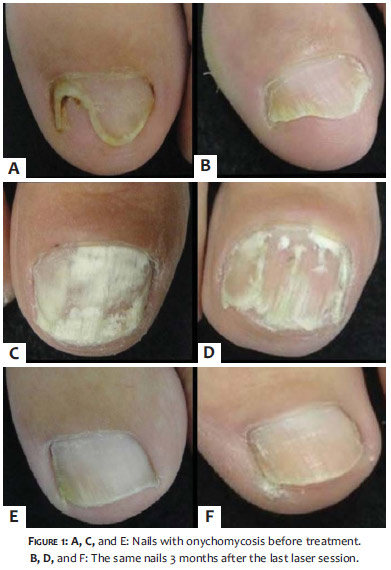
Of the 19 nails analyzed, 12 (63%) showed improvement in the affected area, 3 (16%) remained unaltered and 4 (21%) showed increased fungal infection. When there was an improvement of the affected area, it varied between 20-60% (mean value = 43.7%). (Figure 1)
The nails that presented negative results in the mycological examination also had clinical improvement. (Table 2)
Due to the limitations of treatments for onychomicosis, some studies have demonstrated the use of laser for that purpose with promising results.4,7,8 Among its benefits are: a shorter treatment duration, a low rate of occurrence of local adverse effects, the absence of systemic adverse effects, and a high patient adherence.
The present study demonstrated clinical improvement in 63% of the treated patients 3 months after the last session. The mean improvement in the affected area was 43.7%.
Poor response was observed in the nails that presented important initial pachyonychia, with that being possibly considered a limiting factor for the laser in reaching the fungal wall, and also suggesting the necessity of further studies on the need of ungual abrasion prior to treatment.
Depending on the angle of the nail bed, the coupling of the tip may have compromised the outcome in patients with predominantly lateral onychomycosis, which was already considered as having the worst prognosis.
There are no studies that are encompassing enough to establish the optimal number of sessions, the parameters to be used in the laser application, and the most appropriate thickness of the nail plate for obtaining better results. Future research may provide more reliable data for effective treatment of onychomycosis through the method described in the present paper.
The present study corroborates the current data from the literature on the potential use of 1,064 nm Nd:YAG laser for the safe and effective treatment of onychomycosis. The optimal treatment regimen remains to be defined and further research is needed to verify whether the complete clinical cure can be achieved with this therapeutic modality. For now, the laser-based treatment constitutes an option for those patients with contraindications to standard treatments, due to its absence of significant adverse effects, ease of application, and good patient acceptance.
1. Gupta AK, Jain HC, Lynde CW, Macdonald P, Cooper EA, Summerbell RC. Prevalence and epidemiology of onychomycosis in patients visiting physicians'offices: a multicenter Canadian survey of 15000 patients. J Am Acad Dermatol. 2000;43(2 pt 1):244-8.
2. Erbagci Z, Tuncel A, Zer Y, Balci I. A prospective epidemiologic survey on the prevalence of onychomycosis and dermatophytosis in male boarding school residents. Mycopathologia 2005;159(3):347.
3. Weinberg JM, Koestenblatt EK, Tutrone WD, Tishler HR, Najarian L. Comparison of diagnostic methods in the evaluation of onychomycosis. J Am Acad Dermatol. 2003;49(2):193-7.
4. Gupta AK, Uro M, Cooper EA. Onychomycosis Therapy: Past, Present, Future. J Drugs Dermatol. 2010;9(9):1109-13.
5. Thomas J, Jacobson GA, Narkowicz CK, Peterson GM, Burnet H, Sharpe C. Toenail onychomycosis: an important global disease burden. J Clin Pharm Ther. 2010;35(5):497-519.
6. Gupta AK, Ryder JE, Johnson AM. Cumulative meta-analysis of systemic antifungal agents for the treatment of onychomycosis. Br J Dermatol 2004;150(3):537-44.
7. Hochman LG. Laser treatment of onychomycosis using a novel 0,65- millisecond pulsed Nd:YAG 1064-nm laser. J Cosmet Laser Ther. 2011;13(1):2-5.
8. Vural E, Winfield HL, Shingleton AW, Horn TD, Shafirstein G. The effects of laser irradiation on Trichophyton rubrum growth. Lasers Med Sci 2011;23(4):349-53.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}