


Elimar Elias Gomes1; Tatiana Cristina Moraes Pinto Blumetti1; Mariana Petaccia de Macedo2; Marcela Pecora Cohen3; Maria Dirlei Bergami2; Gisele Gargantini Rezze1
Early diagnosis of basal cell carcinoma-a cutaneous neoplasia with high incidence-can bring great benefits to the patient. Often, slightly pigmented lesions, small initial lesions, and superficial lesions can represent a clinical and dermoscopic diagnostic challenge for not having the typical findings of this neoplasia. In such cases, optical coherence tomography-a promising technology in dermatology-is an auxiliary, non-invasive resource that can be incorporated into the clinical practice.
Keywords: BASAL CELL CARCINOMA, DIAGNOSTIC IMAGING, OPTICAL COHERENCE TOMOGRAPHY.
Basal cell carcinoma (BCC) is the most common malignancy in the fair-skinned Caucasian population. Its morbidity results from the invasion and destruction of local tissues, rarely causing metastases. Epidemiological data show increasing incidence, even affecting young people.1 The importance of early diagnosis is in its value for targeting the best treatment option, leading to less operative morbidity, lower costs, lower recurrence rates, and better patient prognosis. Often easy to identify at a clinical examination, BCC is difficult to diagnose-especially in early, small, and superficial lesions.
In the last two decades there has been a progressive increase in the number of non-invasive techniques to assist in the early diagnosis of skin lesions, such as dermoscopy, in vivo confocal microscopy, and optical coherence tomography (OCT),2 a promising imaging diagnostic technique, which provides images of the morphology of biological tissues in vivo and in real time with micro-resolution power. It was first described in dermatology by Welzer et al. (1997) and has since been offering advances in technical and image resolution.3 This technology is based on the physical principle of interferometry, and its functionality is analogous to that of the ultrasound. However, with this technology the ultrasound pulses are replaced by a low-coherence source of light, with a wavelength of 1,300nm (close to infrared frequency). An optical system allows for the acquisition of images-in black and white, in two or three dimensions, and perpendicular to the skin's surface-similar to those obtained by histology, and without causing harm to the patient.3,4
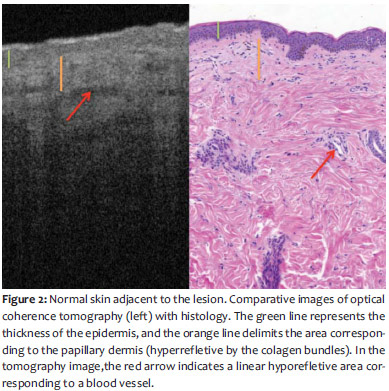
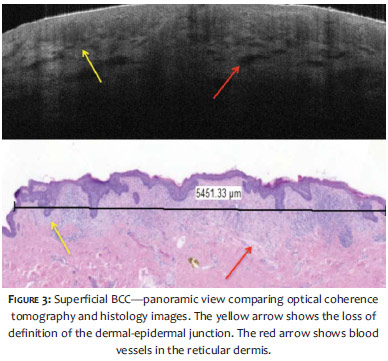
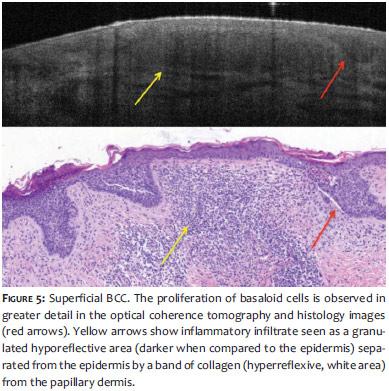
A thirty-eight-year-old female patient, phototype 3, complained of an erythematous lesion in the right sternum region, which had arisen six months before. At the examination, she showed an erythematous, shiny scaly plaque, roughly 7.0 mm in diameter. Through dermoscopy, a lesion with rosy background, no evident pigmentation, and the presence of short linear vessels distributed throughout the lesion could be observed (Figure 1). Based on the clinical and dermoscopic aspects, the main diagnosis was that of a superficial BCC. In the absence of conclusive dermoscopic criteria for the diagnosis of BCC, the differential diagnoses of actinic keratosis, squamous cell carcinoma in situ, and dermatosis of inflammatory character could not be discarded. In an attempt to elucidate the case, the authors decided to carry out an optical coherence tomography using the OCT Vivosight© device (Michelson Diagnostics, Orpington, England, UK). During this examination, unlike the normal structure of the skin shown in Figure 2, they observed a complete disorganization of the dermal-epidermal junction (Figure 3). In some areas it was possible to observe hyporeflective blocks (darker) contiguous with the epidermis and projecting towards the superficial dermis (Figures 4 and 5). It was still possible to identify hyporeflective areas modifying the structure of the papillary dermis, which can correspond to inflammatory infiltrate. It was also possible to identify dark linear areas in the reticular dermis that correspond to vascular proliferation (Figure 5). In light of these findings, which were consistent with the description of BCC already published in the literature, the patient underwent surgical excision of the lesion with safety margins. The anatomical pathological examination confirmed the superficial BCC diagnosis, free of neoplastic involvement of resection margins.
Inexpensive, easy to perform, and widely disseminated, dermoscopy has become an indispensable tool for dermatological evaluation, promoting a significant increase in the sensitivity of the clinical examination for early detection of various cutaneous neoplasias.2
In 2000, Menzies et al. developed a model for the dermoscopic diagnosis of pigmented BCC that showed a sensitivity of 97% and a specificity of 93%. 5 This model was based on the absence of a pigmentary network and the presence of at least one of the following dermoscopic features: ulceration, large blue-grayish ovoid nests, multiple blue-grayish globules, leafshaped areas, wheel spokes areas and arboriform telangiectasia. In 2010, Altamura et al. retrospectively studied 609 cases of various histological subtypes of BCC, pigmented or not, and assessed the variability and diagnostic relevance of diverse dermatoscopic findings.6 In that study, the findings reported by Menzies were deemed classic BCC dermoscopic patterns, with other dermoscopic findings, called non-classic, having been included.5,6 The findings described as non-classic were very short, superficial telangiectasias, small multiple erosions, concentric structures, and nests of multiple blue-grayish dots.6 In this context, lightly pigmented, initial and superficial BCC lesions may represent a clinical and dermoscopic diagnostic challenge due to the fact that they do not present dermoscopic findings typical of BCCs.
The OCT is a non-invasive, quick, and easy to perform examination. Images obtained are perpendicular to the skin, similar to the standard histological specimens, which facilitates interpretation. Widely used in other medical areas such as ophthalmology, cardiology, and gastroenterology, this new technology has only recently been introduced in dermatology. Nevertheless it has already yielded promising results in the differential diagnosis of non-melanoma cutaneous tumors.3,4
The first studies on the pattern of BCC images in optical coherence tomography are recent and show a loss of the normal architecture of the different skin layers and structures resembling hyporeflective tumor blocks (darker when compared to epidermal tissue) surrounded by dark silhouettes (linear areas close to the black color). These findings were correlated with histology, corresponding to basaloid tumor cells blocks, characteristic of this neoplasm. The dark silhouettes correspond to the slit surrounding the tumor blocks, and the presence of a white band encircling the darkened lobes corresponds to the tumoral stroma.4,7-9
In a study carried out by Mogensen et al., the main features observed in tomography's images of BCC were the loss of lamellar structure in the epidermis (mainly in the superficial BCCs), focal alterations of the epidermis with white striae and dots in some lesions, and lobular grayish or darkened structures surrounded by whitish borders.10
In the present case, the OCT showed findings consistent with those described in the literature for this new technology. This fact indicates the reproducibility of the examination, the good histological correlation and, more importantly, it has brought benefits to the patient since it avoids incisional biopsy, reducing costs and streamlining the definitive treatment.
1. Christenson LJ, Borrowman TA, Vanchon CM, Tollefson MM, Otley CC, Weaver AL, et al. Incidence of basal cell and squamous cell carcinomas in population younger than 40 years. JAMA. 2005;294(6):681-90.
2. Di Giacomo THB, Santiago AVD, Braga JCT, Blumetti TCMP, Ferreira JASLB, Canosa JM, et al. Perspectivas no uso da microscopia confocal in vivo na prática do cirurgião dermatológico. Surg Cosmet Dermatol. 2011;3(4):338-44.
3. Welzel J, Lankenau E, Birngruber R, Engelhardt R. Optical coherence tomography of the human skin. J Am Acad Dermatol. 1997;37(6):958-63.
4. Schmitz L, Reinhold U, Bierhoff E, Dirschka T. Optical coherence tomography: its role in daily dermatological practice. J Dtsch Dermatol Ges. 2013;11(6):499-507.
5. Menzies SW, Westerhoff K, Rabinovitz H, Kopf AW, McCarthy WH, Katz B. Surface microscopy of pigmented basal cell carcinoma. Arch Dermatol. 2000;136(8):1012.
6. Altamura D, Menzies SW, Argenziano G, Zalaudek I, Soyer HP, Sera F, et al. Dermatoscopy of basal cell carcinoma: Morphologic variability of global and local features and accuracy of diagnosis. J Am Acad Dermatol. 2010;62(1):67-75.
7. Olmedo JM, Warschaw KE, Schmitt JM, Swanson DL. Optical coherence tomography for the characterization of basal cell carcinoma in vivo: a pilot study. J Am Acad Dermatol. 2006;55(3):408-12.
8. Cohen PR, Schulze KE, Nelson BR. Basal cell carcinoma with mixed histology: a possible pathogenesis for recurrent skin cancer. Dermatol Surg. 2006;32(4):542-51.
9. Gambichler T, Orlikov A, Vasa R, Moussa G, Hoffmann K, Stücker M, et al. In vivo optical coherence tomography of basal cell carcinoma. J Dermatol Sci. 2007;45(3):167-73.
10. Mogensen M, Joergensen TM, Nürnberg BM, Morsy HA, Thomsen JB, Thrane l, et al. Assessment of Optical Coherence Tomography Imaging in the Diagnosis of Non-Melanoma Skin Cancer and Benign Lesions Versus Normal Skin: Observer-Blinded Evaluation by Dermatologists and Pathologists. Dermatol Surg.2009;35(6):965-72.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}