


Flávia Alvim Sant'Anna Addor1; Patrícia Camarano2; Christiane Agelune3
Introduction: UV light-induced photodamage is an acute precipitator of solar erythema, which is the phenomenon measured to assess the protection against the sun provided by a particular product. Objective: To investigate the ability of a dietary supplement containing antioxidants (carotenoids, trace elements/oligoelements, flaxseed oil, and vitamins E and C) to prevent photodamage, using as a parameter the minimum erythema dose level. Method: The minimum erythema dose level of 28 volunteers (Fitzpatrick skin types 2 and 3) was measured with a solar simulator, before and after 30 and 60 days of supplement use. Results: The daily use of the supplement was well tolerated. There was a significant increase in the minimum erythema dose level in the group evaluated (p = 0.017). Conclusion: The studied combination of antioxidants was demonstrated to increase the minimum erythema dose level with statistical significance, suggesting the presence of photoprotective activity.
Keywords: ULTRAVIOLET RAYS, ANTIOXIDANTS, CAROTENOIDS.
Exposure to the ultraviolet range of solar radiation induces erythema and pigmentation that vary according to skin phototype.1
Solar-induced erythema occurs mainly in fair-skinned individuals, beginning two to four hours after sun exposure and reaching its greatest intensity after roughly 24 hours. It results from vasodilation and subsequent migration of polymorphonuclear leukocytes, characterizing an acute inflammatory reaction. Ultraviolet B radiation is the main determinant of the occurrence of erythema.2
Some standardized resources are used in the literature for quantifying individual susceptibility to erythema. The minimal erythema dose (MED) is defined as the lowest effective erythematogenic energy amount (i.e. sufficient to produce the first perceptible erythema reaction with defined borders). In order to determine the MED, the individual must be exposed to increasing doses of ultraviolet radiation generated by a device called Solar Simulator, which has a radiation spectrum similar to that of the sun. The reading of the erythema is carried out 24 hours after the exposure, with the MED being subsequently determined.3
The higher the MED, the greater the individual's resistance to the production of erythema.
The determination of the Individual Typological Angle-ITA-an index that relates to skin color, is calculated using measurements obtained from a colorimeter.4
The prevention of erythema is desired by individuals with acute sun exposure, given its obvious discomfort. In addition to topical sunscreens, certain oral agents may have photoprotective action, increasing the MED through antioxidant or anti-inflammatory mechanisms, since the pigmentation results from the melanin photooxidative process.
The association of nutrients with antioxidant and antiinflammatory action can be beneficial in preventing erythema.5 One way to evaluate the effect is by determining the MED 6 before and after the use of the supplement.
The present study was aimed at evaluating the efficacy of a vitamin supplement in reducing erythema, by increasing the MED, which was measured before and after use.
A prospective, controlled, blind, non-comparative study was carried out between April and July 2013, ata private clinical research laboratory, in the city of Osasco, in the Brazilian state of São Paulo.
The study population consisted of 33 adult female patients between 18 and 60 years old, with Fitzpatrick skin phototypes II and III. Patients using immunosuppressive or anti-inflammatory drugs, individuals with photodermatosis history, and pregnant and lactating women were excluded.
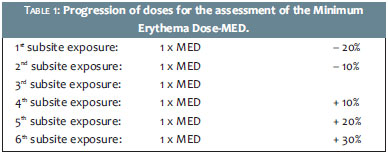
After signing the term of free and informed consent, all participating volunteers were evaluated clinically and had their inclusion and exclusion criteria checked. Subsequently, colorimetry measurements were taken with the colorimeter (Konica Minolta CR400, UK) on each patient's dorsum, the area chosen for testing the ITA and then the Ultraviolet B radiation. In this manner, the patient's dorsal area was divided into six sites, with each being irradiated with progressive doses emitted by a solar simulator. The doses were predetermined using a UVB irradiation detector, with each dose being 12% higher than the previous one, following a geometric progression. This irradiation progression is the same as that recommended in the methodology for determining the sun protection factor.7
The solar simulator (Solar Light,® Solar Light Co, Glenside, PA, USA) is a device capable of emitting light in the range of the solar spectrum, and is a reference in studies aimed at determining sun protection factor (SPF) and other studies in photobiology, complying with the European and North American technical requirements regarding photoprotection directives.
The median dose (4th subsite exposure) corresponds to the MED, being thus defined based on the value obtained through the calculating of the ITA. The remaining doses were determined through the geometric progression, as shown below (Table 1).
After the exposure, the volunteer was observed for 15 minutes for possible immediate reactions to ultraviolet radiation, such as tanning, reflex erythema, and vesicular eruptions. After the 15-minute observation, patients were discharged and instructed to come back after 24 hours for an assessmentof the test area.
After the assessment, 24 hours later, when the MED was determined through the analysis of the erythema using standardized lighting intensity, the volunteers received a sample of the vitamin supplement and were instructed to ingest one capsule per day.
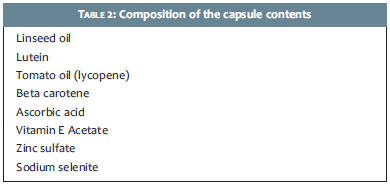
Table 2 shows the content composition of each capsule.
The supplement was ingested in this dose for eight weeks. New measurements of the MED following the same standards were carried out after four and eight weeks, when the study ended.
Of the 33 invited and included volunteers, 28 completed the study. Four dropped out for reasons unrelated to the protocol, and one was excluded due to the use of a medication not allowed during the study.
None of the volunteers showed any adverse reaction related to the supplement use during the study period.
The statistical evaluation of the results was performed using the Student's t-test, with a significance level of 5% (p = 0.05).
Evaluation of the Minimal Erythema Dose
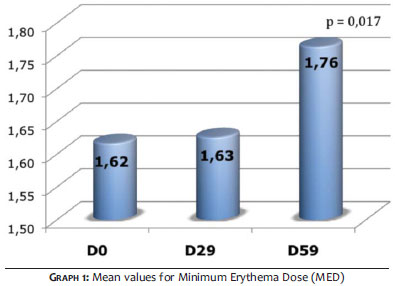
Graph 1 shows the evolution of the mean values of the MED at intervals (in days) T0, T30 and T60. From Graph 1, it can be concluded that the daily use of the supplement led to a statistically significant increase (p = 0.017) in the MED values as from 60 days. An important finding is noteworthy: four volunteers did not exhibit erythema in any of the irradiation sessions, suggesting there was considerable increase in the MED, even with increases of up to 30% in the irradiation amount.
The combination of oral antioxidants as agents for reducing photodamage, based on increased levels of MED, is already known. In addition, the photoprotective effect of topical-or even systemic antioxidants-has already been demonstrated in several experimental studies.8,9
A clinical trial using the combination of vitamins E (in 500 IU doses) and C (in 1g doses) twice a day, showed a significant increase in MED from 90 days.10
The concomitant use has superior results, even reducing the formation of thymine dimers, what has been demonstrated in animal models.11
The synergistic effect among antioxidants is possible and can lead to increased quality of the protective effect not only against the immediate photodamage, but also against cellular phenomena typical of photodamage.12
The association of nutrients can also allow for the use of lower, alimentary doses, thus preventing effects such as hypervitaminosis.13
The oral supplementation evaluated in the present study combined antioxidants with diverse mechanisms, meaning that the protective effect can be enhanced as well as having an earlier action, which can be observed as from 60 days of use.
Molecules, such as lutein and lycopene, already established as oral antioxidants with photoprotective effect, 14,15 may act in tandem, potentializing the antioxidant effects. Lycopene, for instance, can be associated with another carotenoid, with no competition in the absorption and utilization or pro-vitamin A activity. None of these is the human body not able to synthesize. 16
Linseeds are rich in essential fatty acids, fiber, and phenolic compounds. These compounds exert antioxidant activity, being a significant source of essential fatty acids ω-3 and ω-6, both of which are crucialin the maintenance of the skin barrier and modulation of inflammatory activity.17
Minerals such as zinc and selenium are factors that constitute the fundamental enzymes for the antioxidative mechanism-such as superoxide dismutase and glutathione peroxidase, respectively. 18, 19
The combination of nutrients with antioxidant value has the ability to provide protection against acute photodamage, measured in the present study through the increase in the Minimal Erythema Dose. Concentrations in dietary doses have an adequate safety profile, avoiding the risk of toxicity.
2. Soter NA. Acute effects of ultraviolet radiation on the skin. Seminars in Dermatology. 1990;9(1):11-5.
3. Azizi E, Lusky A, Kushelevsky AP, Shewach-Millet M. Skin type, hair color, and freckles are predictors of decreased minimal erythema ultraviolet radiations dose. J Am Acad Dermatol. 1988;19(1 pt 1):32-8.
4. Chardon, A, Cretois I, Hourseau. Skin Colour Typology and Suntanning Pathways. Int J Cosmet Sci. 1991;13(4):191-208.
5. Steenvoorden DP, van Henegouwen GM. The use of endogenous antioxidants to improve photoprotection. J Photochem Photobiol B. 1997;41(12):1-10.
6. Jocher A, Kessler S, Hornstein S, Monting JS, Schempp CM. The UV Erythema Test as a Model to Investigate the Anti-Inflamatory Potency of Topical Preparations - Reevaluation and Optimization of the Method. Skin Pharmacol Physiol. 2005;18(5):234-40.
7. International Sun Protection Factor (SPF) Test Method. JCIA, COLIPA, CTFA. 2006.
8. Eberlein-Ko¨ nig B, Placzek M, Przybilla B. Protective effect against sunburn of combined ascorbic acid (vitamin C) and D-a-tocopherol (vitamin E). J Am Acad Dermatol. 1998;38(1):45-48.
9. Pinnell SR. Cutaneous photodamage, oxidative stress, and topical antioxidant protection. J Am Acad Dermatol. 2003;48(1):1-19.
10. Placzek M, Gaube S, Kerkmann U, Gilbertz KP, Herzinger T, et al. Ultraviolet B-Induced DNA Damage in Human Epidermis Is Modified by the Antioxidants Ascorbic Acid and D-a-Tocopherol. J Invest Dermatol. 2005;124(2):304-7.
11. Lin J-Y, Selim A, Shea C, Grichnik JM, Omar MM, Monteiro-Riviere NA, et al. UV photoprotection by combination topical antioxidants vitamin C and E. J Am Acad Dermatol. 2003;48(6):866-74.
12. Lima XT, Alora-Palli MB, Beck S, Kimball AB. A double-blinded, randomized, controlled trial to quantitate photoprotective effects of an antioxidant combination product. J Clin Aesthet Dermatol. 2012;5(4):29-32.
13. Cornelli, U. Antioxidant use in nutraceuticals. Clin Dermatol. 2009;27(2):175-94.
14. Pongcharoen S, Warnnissorn P, Leŗtkajornsin O, Limpeanchob N, Sutheerawattananonda M. Protective effect of silk lutein on ultraviolet Birradiated human keratinocytes. Biol Res. 2013;46(1):39-45.
15. Rizwan M, Rodriguez-Blanco I, Harbottle A, Birch-Machin MA, Watson RE, Rhodes LE. Tomato paste rich in lycopene protects against cutaneous photodamage in humans in vivo: a randomized controlled trial. Br J Dermatol. 2011;164(1):154-62.
16. Johnson EJ, Qin J, Krinsky NI, Russell RM. Ingestion by men of a combined dose of betacarotene but improves that of lycopene. J Nutr. 1997;127(9):1833-7.
17. Addor, F.A.S. Abordagem nutricional de envelhecimento cutâneo: correlação entre os efeitos em fibroblastos e os resultados clínicos. Surg Cosmet Dermatol. 2011;3(1):12-6.
18. Al-Sheikh YA, Ghneim HK. The effect of micronutrients on superoxide dismutase in senescent fibroblasts. Cell Biochem Funct. 2011;29(5):384-93.
19. Sokmen BB, Basaraner H, Yanardag R. Combined effects of treatment with vitamin C, vitamin E and selenium on the skin of diabetic rats. Hum Exp Toxicol. 2013;32(4):379-84.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}