


Flávia Naranjo Ravelli1, Jayme de Oliveira Filho1, Nilceo S. Michalany1, Irina Andrea Pires Afonso1, Thais Berti Franchin1, Ana Carolina Lisboa de Macedo1
Keywords: NEUROMA, SKIN NEOPLASMS, SCHWANN CELLS
In 1972, Reed et al. described forty-four cases of a different type of neural tumor, which they denominated palisaded encapsulated neuroma of the skin (PEN), also known as solitary circumscribed neuroma.1-3 It is a solitary neural tumor of the skin, meaning it is not associated with other stigmata of neurofibromatosis. It is encapsulated and characterized by the presence of compact bundles of parallel fascicles of Schwann cells.1
It is clinically characterized by slow growth, and occurs mainly on the face of men and women aged 30-60 years.1,2 The typical lesion is a solitary, painless, non-pigmented papule or sessile papule-nodule, which arises in the central facial region.1,2 It constitutes a rigid and firm lesion that when examined through palpation, appears to be in the dermis.1 When pressed, it does not suffer herniation into the dermis, as is the case with neurofibromas.1The skin on the tumor is smooth and pearly, and seems as if it is being stretched by the pressure of the subjacent tumor.1 Telangiectasia can be present in the lesion, but they are not prominent or common-as they are with basal cell carcinomas (BCC). 1 Terminal hair is rarely observed in this tumor, contrary to what is found in some nevi.1,2
Histologically, the neoplasia appears confined to the dermis and partially or completely surrounded by dense fibrous tissue that forms a capsule.1,2 When properly formed, that capsule resembles the perineurium and, in some sections presents itself in continuity with it, being stained with epithelial membrane antigen (EMA).1,2 Some of these tumors are separated from the epidermis by a band of normal dermis, however others extend to the epidermis, which may present acanthotic.1,2 The lesion is formed by numerous fusiform fascicles of Schwann cells with eosinophilic cytoplasm that stain intensely for protein S100.2 These fibers are characteristic of neural tumors and are described as "wire-like" due to their spatial arrangement.1
The main differential diagnoses of the PEN are: BCC, chondrodermatitis nodularis helix, pyogenic granuloma, leiomyoma, chalazion, neurofibroma, seborrheic keratosis, actinic keratosis, cysts, sebaceous adenoma, trichofoliculoma, eccrine spiradenoma, fibrous papulae of the face, nevus and verruca vulgaris.1-3
A white, 55-year-old female patient being treated at a private practice, reported a long history of asymptomatic hypochromic macula in the right supralabial region. Slow growth had been noticed in recent months, with the transformation of the lesion into a beige circular papule, with a smooth and dome-shaped surface, which had fine telangiectasias (on the surface), simulating a BCC (Figure 1). The therapy chosen was exeresis and suture of the lesion, followed by anatomical histological examination (AP).
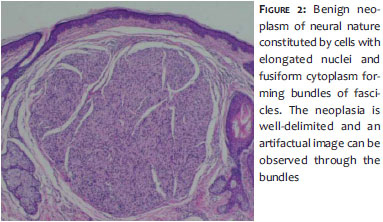
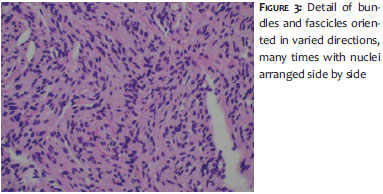
Observed was a benign, well-delimited neoplasia of neural nature constituted by cells with elongated nuclei and fusiform cytoplasm forming bundles and fascicles oriented in various directions, often with nuclei arranged side by side. The supra-adjacent epidermis appeared tapered, with rectification of interpapillary crests (Figures 2 and 3).
Benign tumors of the nerve sheath are divided into three categories: schwanommas (neurilemmomas), neurofibromas, and true neuromas.1 The absence of axons in most schwanomma cases, allows its differentiation from the other two categories.1 However, the differentiation between neurofibromas and neuromas is more difficult to attain.1 The presence of axons is shown in some or many of the fascicles of Schwann cells in neurofibromas, however the proportion of axons as compared to fascicles is not anywhere near 1:1.1Yet in true neuromas, this relationship approximates the ratio of 1:1.1
The PEN of the skin is a benign, well-circumscribed, solitary tumor most often found on the face of middle-aged adults.1,2 Nonetheless, these lesions have also been described in other body regions, such as the trunk, shoulder, arm, hand, foot, oral mucosa, nasal cavity, and glans penis.1,2 It can be easily mistaken for BCC, melanocytic nevus, epidermal cysts, or tumors of skin appendages.1-3
The long duration of the tumor, the sparse telangiectasias and the absence of ulceration assist in the differentiation from BCC, while distinction from nevus is done through analyzing the lesion's rigidity and the absence of terminal hair, which can be observed in PEN.1-3 However, the differentiation from tumors of skin appendages is extremely difficult, often only being performed through histologic analysis.1,2
Histologically, PEN is a well-circumscribed and encapsulated tumor that has interwoven fusiform fascicles, usually separated by artifactual clefts.2 Tumor cells stain positively for S100 protein, type IVcollagen, and vimentin, which show staining in Schwann cells.2 The lesion's capsule contains perineural cells that stain positively for EMA.2
True solitary and spontaneous neuromas are rare, and seldom reported. In the authors' opinion, having knowledge of this entity is key for carrying out differential diagnosis against other lesions, especially with BCC, tumors of skin appendages, nevi, and epidermal cysts.
1. Reed RJ, Fine RM, Meltzer HD. Palisaded, encapsulated neuromas of the skin. Arch Dermatol. 1972; 106(6):865-70.
2. Dubovy SR, Clark BJ. Palisaded encapsulated neuroma (solitary circumscribed neuroma of skin) of the eyelid: report of two cases and review of the literature. Br J Ophthalmol. 2001. 85(8):949-51.
3. Dover JS, From L, Lewis A. Palisaded encapsulated neuromas. Arch Dermatol. 1989;125(3):386-9.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}