


Michelle dos Santos Diniz1, Daniel Gontijo Ramos1, Mauricio Buzelin Nunes1
Keywords: DERMATOFIBROSARCOMA; SARCOMA; MOHS SURGERY
Dermatofibrosarcoma protuberans (DFSP) is a spindle cell neoplasm of unknown etiology, first described in 1890 by Taylor, and as a distinct entity by Darier and Ferrand in 1924. It is an uncommon tumor with an incidence rate of 0. 8 to 5 cases per million inhabitants/year, corresponding to less than 0. 1% of all malignancies and to approximately 1% of soft tissue sarcomas. Most studies have found similar incidence rates in both genders. Some, however, have showed a predominance in men, with DFSP occurring up to four times more frequently in that group, especially in elderly patients. The most affected age group is 3050 year-olds.1-7
The most common site of occurrence is the trunk (40-60%), followed by the limbs (20-30%), and head and neck (10-15%). When occurring on the scalp and in the supraclavicular region, the tumors are associated with higher morbidity and an increased risk of local recurrence.1,4,6
The tumor is clinically characterized by a skin-colored papule or plaque, erythematous or yellowish, and usually asymptomatic. Areas of atrophy, induration, or telangiectasia may be present from the outset or arise with the development of the tumor. Growth is slow, infiltrative, with high rates of local recurrence, however with low rates of metastases.1-6,8
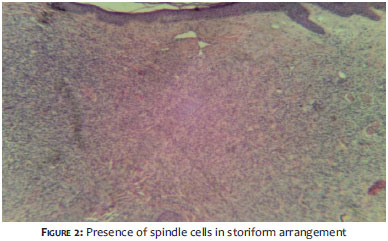
Histological characteristics that suggest DFSP are a dense and uniform collection of spindle cells with a characteristic storiform arrangement. The stroma has varying amounts of collagen and capillaries. Recent lesions may have areas of untouched dermis or Grenz zone just below the epidermis. The tumor can infiltrate the subcutaneous tissue, distorting the adipose tissue's architecture with a honeycomb appearance. Deep projections towards the fascia and muscle hamper its delimitation and subsequent surgical removal.1,4,6,7
The treatment of DFSP is mainly based on surgical resection, however, in selected cases, radiotherapy and chemotherapy can be used.2
The present paper describes the case of a patient with DFSP in an uncommon location, treated with Mohs micrographic surgery.
A thirty-nine-year-old male patient, living in the city of Belo Horizonte (MG), Brazil, had had an asymptomatic lesion on the forehead for about three years. Physical examination showed a yellowish, well-defined papule of fibrous consistency and 0. 7 cm in diameter, in the right frontal region (Figure 1).
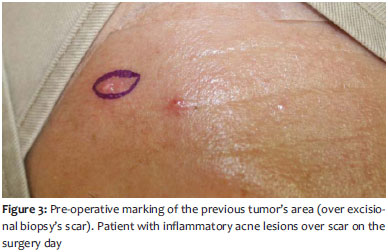
The total excision of the lesion was carried out without surgical margin, revealing undifferentiated spindle cell neoplasm with compromised margins (Figure 2), suggesting immunohistochemistry for diagnosis. Immunohistochemistry resulted positive for CD34, vimentin and Ki 67, being compatible with DFSP. Mohs micrographic surgery was indicated due to the location of the lesion and the risk of tumor recurrence (Figure 3).
Three stages were necessary to complete the excision of the tumor during the Mohs micrographic surgery. The first stage identified tumor involvement at the deep and medial margins, with the increase in margins being made in this direction (Figure 4). The second stage demonstrated the tumor only in the deep margin (Figure 5), and in the third and last stage the deep margin was expanded with removal of muscle tissue, reaching the galea (Figure 6). No histological signs of tumor were identified in that tissue. The closing of the surgical wound was carried out using a type O-T advancement flap, with good aesthetic result (Figure 7). When the present report was written, the patient had four months of post-operative follow up with no signs of local recurrence (Figure 8).
DFSP is a neoplasm of intermediate malignancy and low risk of metastasis. This tumor's high rate of local recurrence, in addition to high morbidity, nevertheless justifies the effort directed towards early diagnosis and the need for initial treatment that allows greater cure rates.
Given that in most cases it is a non-specific and asymptomatic lesion, the initial DFSP may not be perceived by the patient or can be mistaken for a benign lesion.6 The size of the tumor depends on the development time. At diagnosis, it is usually between one and 5cm.1 Cai et al.2 found among a group of 260 studied patients an average tumor size of 3.1 cm at diagnosis. In the case described by the present report, it is important to emphasize that the diagnosis was attained considerably early, given that the tumor was less than 1cm in diameter.
In doubtful cases-as in the present report or in order to confirm the diagnosis-immunohistochemistry analysis must be carried out. CD34 is the most useful marker to differentiate DFSP from other fibro-histiocytic tumors, and its positivity ranges from 92-100%.1,2,6,8 CD34 positivity can, however, be found in other tumors, such as melanoma, neurofibroma and perineuroma. The most important differential diagnosis is against dermatofibroma, which typically is positive for the Factor VIII and negative for CD34.1 Loss of positivity for CD34 can be observed in DFSP with sarcomatous transformation.8
Surgical resection is the primary treatment for patients with DFSP, however simple local excision is not an adequate approach2,4,6 Approximately 50% of patients with wide local excision still present residual tumors in the histology.2
Recurrence rates can reach up to 60% of cases and wide excision can entail a reduction of 10-33%. The factors associated with a higher risk of local recurrence are: histological subtype, mitotic index, cellularity, size and depth of the tumor, location in the head and neck, extension of the surgical margin, and recurrent lesions.2,3,5 Regarding surgical margins, a study showed that patients treated with margins greater than 3cm have a recurrence rate of 5.7%, while those with margins of 1. 5-3 cm had a 13. 6% recurrence rate. This difference was statistically significant.2 Lesions with multiple recurrences after initial treatment seem more prone to dedifferentiation in sarcomas with a high degree of malignancy, resulting in an increased risk of metastasis.3
Mohs micrographic surgery has demonstrated the highest cure rates for this tumor4,9 and should be given serious consideration when there is involvement of the head, neck, face, or hands and feet; locations in which complete resection with the narrowest required margin is the best option to in order to avoid aesthetic and functional damage.2,4 Cure rates reported for head and neck using this method were 91.2%. A 94% rate was obtained for the trunk. Other studies have shown recurrence rates even lower than this, in the range 0. 8-3% when employing micrographic surgery.1,3,6 In addition to the higher cure rate, a study showed that the average final defect with traditional surgery and a 3cm margin, was of 17.78 cm2, as compared to a 7.49 cm defect after micrographic surgery.2,3
Other treatments that can be used include radiotherapy and chemotherapy. Conventional chemotherapy has poor results, while that using tyrosine-kinase inhibitors, such as imatinib, entailed partial or complete regression of DFSP in up to two-thirds of patients.1,4,5 Radiation therapy can be indicated in isolation for patients with unresectable macroscopic disease or where wide surgical excision may lead to significant functional and/or aesthetic compromise.1,3-5
The survival rate at five years is roughly 98. 3%, and 95. 7% in ten years.2 Metastases are rare (1-5%) and affect lymph nodes, lungs, and bones. The main prognostic factors are: inadequate surgical removal with positive margins, large tumors located in the head, and the presence of areas of fibrosarcoma in the histology.1
Biopsy of clinically undefined lesions is critical for the early diagnosis of tumors like DFSP. Micrographic surgery offers the highest cure rates with greater tissue preservation in the treatment of DFSP and should be highly considered as the first choice treatment.
1. Serra-Guillén C, Llombart B, Sanmartín O. Dermatofibrosarcoma protuberans. Actas Dermosifiliogr. 2007;98(2):77-87.
2. Cai H, Wang Y, Wu J, Shi Y. Dermatofibrosarcoma protuberans: clinical diagnosis ans treatment results of 260 cases in China. J Surg Oncol. 2012;105(2):142-8.
3. Galimberti G, Montaño AP, Kowalczuk A, Ferrario D, Galimberti R. Outcomes in 11 patients with dermatofibrosarcoma protuberens treated with Mohs micrographic surgery. Int J Dermatol. 2012;51(1):89-93.
4. Johnson-Jahangir H, Ratner D. Advances in management of dermatofibrosarcoma protuberans. Dermatol Clin. 2011;29(2):191-200.
5. Fields RC, Hameed M, Qin LX, Moraco N, Jia X, Maki RG, et al. Dermatofibrosarcoma protuberans (DFSP): predictors of recurrence and the use of systemic therapy. Ann Surg Oncol. 2011;18(2):328-36.
6. Fleury LFF Jr, Sanches JS Jr. Sarcomas cutâneos primários. An Bras Dermatol. 2006;81(3):207-21.
7. Pérez OG, Righetti R,Woskoff A, Amante H. Haga su diagnóstico. An Bras Dermatol. 2010;85(2):245-7.
8. Yamamoto Y, Toyozawa S, Uede K, Oda Y, Nakamura Y, Furukawa F. Clinical and pathological changes in a long-term follow-up case of dermatofibrosarcoma protuberans. J Dermatol. 2011;38(2):203-5.
9. Brewer JD, Roenigk RK, Otley CC. Wide local excision or mohs micrographic surgery for primary dermatofibrosarcoma protuberans. Am J Clin Oncol. 2011;34(5):545-6.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}