


Mariana Hammerschmidt1, Arthur Conelian Gentili1, Themis Hepp1, Maira Mitsue Mukai1
Keywords: PURPURA, HEMOSIDERIM, THERAPEUTICS, HYPERPIGMENTATION
First described in 1901, Schamberg's disease is a progressive pigmentary dermatosis of chronic course that is characterized by reddish-brown, irregular maculae associated with petechiae, resembling grains of cayenne pepper. It is asymptomatic and usually affects the legs, however it can affect the trunk and upper limbs.1,2 The observed lesions appear to be the result of hemosiderin deposits associated with melanic hyperpigmentation. It is believed that there is melanocytic activation secondary to ferric pigment deposition in the dermis.3 Thioglycolic acid peelings have been shown to be a safe and efficient treatment option for dermatoses of ferric origin.4
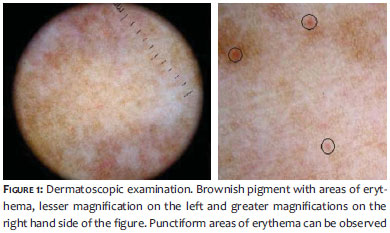
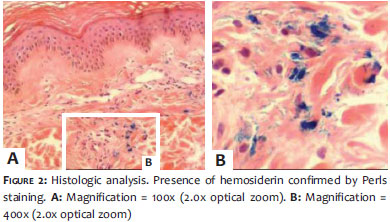
A 43-year-old female patient presented complaining of the sudden onset of stains on the legs and feet, one year earlier. The stains worsened after exposure to the sun. The patient denied comorbidities and use of medication. The examination showed irregular brownish maculae-some confluent-in the legs and dorsum of the feet, bilaterally. The dermoscopy of the lesion evidenced a brownish pigment with areas of erythema (Figure 1). The histologic analysis (Figure 2) showed an increase of melanin pigment in the keratinocytes, as well as dermis with edema and discrete perivascular lymphohistiocytic inflammatory infiltrate with the presence of hemosiderin-evidenced by Perls staining- confirming the diagnosis of Schamberg's disease.
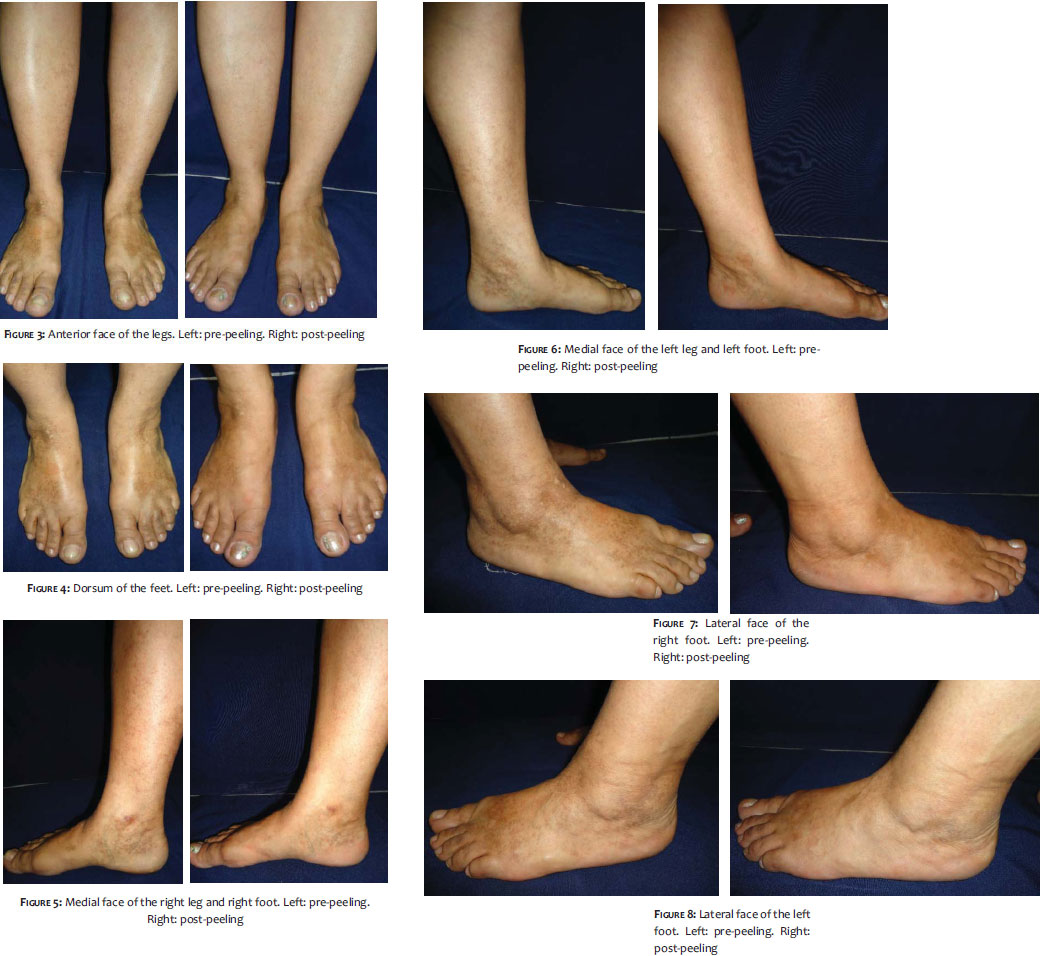
In order to prepare the skin, 10% glycolic acid + 4% hydroquinone + 1% alpha-bisabolol was prescribed for three weeks prior to the procedure. Five sessions of 10% thioglycolic acid (in gel) peeling were carried out at intervals of 15 days. Prior to performing the procedure, it is recommended that the skin be cleansed with a mixture of alcohol, ether and acetone, followed by the application of the acid, which is removed from the skin with soap and water after 20 minutes of contact. The patient did not report pain or any discomfort during the procedure. Slight peeling was observed beginning three days after the procedure, lasting up to ten days. There was a significant whitening of the lesions (Figures 3-8) and patient satisfaction (with a 90% improvement rate reported). Pre- and post- treatment photographic records were evaluated by 20 dermatologists who reported average improvement of 68. 7% (ranging from 5580%). A control biopsy after the fifth session showed an absence of hemosiderin deposition through Perls staining.
The etiology of Schamberg's disease is still unknown.5 Triggering factors-such as hypersensitivity to drugs; and stasis, contact, and factitious dermatitis-were reported.1 Although the exact pathogenesis is unknown, the capillary damage and entailed leakage of erythrocytes, seem to be the result of a lesion mediated by localized immune cells that is induced by a specific subtype of T helper lymphocytes2,6 Histologically, perivascular mononuclear infiltrate can be observed in the upper dermis with extravasation of erythrocytes and hemosiderin deposition, however without fibrinoid necrosis of vessel walls1-a fact verified in the present case. To date, no treatment has demonstrated consistent beneficial effect. There are reports of improvement with topical steroids, griseofulvin, pentoxifylline, PUVA, anti-allergic drugs, colchicine, ascorbic acid, and oral rutosides.1,5,6
The residual stains common to this condition are a cause of distress for many patients, especially women. They seem to be the result of hemosiderin deposits associated with melanic hyperpigmentation, since it is believed that there is melanocytic activation secondary to ferric pigment deposition in the dermis.3
Thioglycolic acid peeling is one of the treatment options for pigmentary disorders of ferric origin.4 Serial and progressive peelings of 10% thioglycolic acid were proven to be a safe, efficient, and cost-effective therapeutic tool in the treatment of constitutional periorbicular hyperpigmentation.7
Thioglycolic acid-also called mercaptoacetic acid-is a representative of the thioglycolates class, and is considered a hemosiderin solubilizing substance.3 Thioglycolates have long been used in the cosmetic industry as components of body epilators, chemical hair straighteners, and hair color.8 Used topically, (from 5-12%) thioglycolic acid has the advantage of not causing pain or redness (sometimes mild), rare sensitization, and only mild and transient desquamation.8 The literature recommends weekly applications, in gel, totaling five to six sessions. The procedure starts with local cleansing, followed by application of the product. The product is left on the skin for a period of 10-30 minutes and is then neutralized with water.8 In the present case, the product was kept on the skin for 20 minutes, without the patients reporting any discomfort. Only mild erythema was observed after applying the product. The authors decided on biweekly sessions, given that mild desquamation occurred for up to ten days after the application sessions. The result obtained was significant, with the complete whitening of the stains in the lower third of the legs and on much of the dorsum of the feet (68. 7% improvement) with high patient satisfaction. The absence of hemosiderin in the control biopsy may indicate a positive response to the treatment, since the sample was collected near the area of the previous biopsy, where there were previous stains. Despite the chronicity of the condition and probable recurrence of the lesions in the long-term, thioglycolic acid peeling was proven to be an efficient tool in the whitening of the lesions, with good tolerance and few side effects.
1. Torrelo A, Requena C, Mediero IG, Zambrano A. Schamberg's purpura in children: a review of 13 cases. J Am Acad Dermatol. 2003;48(1):31-3.
2. Chatterjee S. Schamberg disease: uncommon reaction to a common drug. CMAJ. 2009;181(12):E275.
3. TulliR, Izzo M. El papel del ácido tioglicólico em las pigmentaciones férricas. Rev Panam Flobol Linfol. 2001;41(2):57-63.
4. Izzo M, Verzella G, inventors; I. V. PHARMA S. A. S, assignee. The use of thioglycolic acid as depigmenting agent. patent WO/1998/047466. 1998 October 29. Available from: http://www.freepatentsonline.com/WO1998047466.html
5. Reinhold U, Seiter S, Ugurel S, Tilgen W. Treatment of progressive pigmented purpura with oral bioflavonoids and ascorbic acid: an open pilot study in 3 patients. J Am Acad Dermatol. 1999; 41(2 Pt1):207-8.
6. Geller M. Successful novel treatment of Schamberg's purpura with colchicines. Einstein. 2004; 2(3):206-7.
7. Costa A, Basile AVD, Medeiros VLS, Moisés TA, Ota FS, Palandi JA, et al. 10% thioglycolic acid gel peels: a safe and efficient option in the treatment of constitutional infraorbital hyperpigmentation. Surg Cosmet Dermatol. 2010;2(1):29-33.
8. Burnett CL, Bergfeld WF, Belsito DV, Klaassen CD, Marks JG Jr, Shank RC, et al. Final amended report on the safety assessment of Ammonium Thioglycolate, Butyl Thioglycolate, Calcium Thioglycolate, Ethanolamine Thioglycolate, Ethyl Thioglycolate, Glyceryl Thioglycolate, Isooctyl Thioglycolate, Isopropyl Thioglycolate, Magnesium Thioglycolate, Methyl Thioglycolate, Potassium Thioglycolate, Sodium Thioglycolate, and Thioglycolic Acid. Int J Toxicol. 2009;28(4 Suppl):68-133.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}