


Marcia Regina Monteiro1
Keywords: BLOOD PLATELETS, DERMATOLOGY, BLOOD
The use of Platelet-Rich Plasma (PRP) in medicine has become increasinglymore widespread during the last decade. Most studies on the subject are carried out in areas such as orthopedics, sports medicine, and odontology. Only recently have articles relating to the dermatologic field begun to be published, where PRP has been used in order to promote accelerated wound healing and as an adjuvant treatment in rejuvenation, alopecia, and even following laser sessions.
The main objective of the present article is to describe what PRP is and to introduce some existing publications related to dermatology.
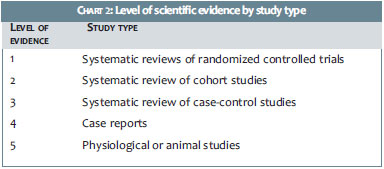
The authors have classified the publications according to the Oxford Centre for Evidence-Based Medicine's guideline1,2 for levels of scientific evidence (LOE), criteria also adopted by the Brazilian Ministry of Health as a standard for the development of technical-scientific opinions (Chart 1).3
The definition of LOE employed in the present article1 takes into account the methods used in the studies and was elaborated with the aim of assisting physicians in making treatment decisions based on the available scientific literature.
Finally, it is important to emphasize that, in response to a request from ANVISA (the Brazilian National Health Surveillance Agency), the Brazilian Federal Council of Medicine (CFM) issued an opinion on the use of PRP, in July 2011. The opinion was requested following media reports highlighting the effects of this therapy in orthopedics and dermatology. The opinion, which is available in its full version on the CFM's website4, states: "Platelet-rich plasma has been used by some physicians with varying results. Due to the variety of such results, it is not yet possible to define the degree of usefulness or approve definitively its use in therapeutic practice, thus it continues to be considered an experimental procedure."
Platelet-rich plasma: what is this?
The term Platelet-Rich Plasma is a generic term used to describe a plasma suspension obtained from whole blood, prepared so as to contain platelet concentrations higher than those normally found in circulating blood. There is no consensus regarding which above-referenced concentration levels define the PRP-reference values used to define normality in the platelet count in blood is 1.5 to 4 x 105 platelets per ml).
A consensus on the appropriate values for classifying a plasma sample as PRP has not yet been reached among researchers, resulting in one of the difficulties found in the evaluation and comparison of results described in scientific articles. There are researchers concerned with obtaining a standardization for these blood derivatives taking into account quantities of components in the PRP, in addition to the platelets themselves.5
It is known that PRP contains diverse concentrations of white and red cells, and that this may have an impact on the final outcome of the proposed treatment.
In 2008, the Brazilian Ministry of Health published a guide for the use of hemocomponents6, where the platelet concentration used for transfusion should contain 1x 107/µl.
Some studies7,8 diverge regarding cellular content and growth factors in PRPs obtained from the same individual when different methods are employed (e. g. one versus two centrifugation cycles). Such divergence was also found when different commercial kits were used in the preparation of blood samples.7 Significant differences in the PRP's final result were also observed in the same individual who underwent successive blood collections.8
There are a number of protocols described for obtaining PRP,9,10 however all in general include a centrifugation process through which the different components of whole blood are separated according to their different densities.
The protocols differ in time, speed, and number of centrifugations to which the whole blood is subjected. The volume of the initial blood sample and the types of collection tubes and anticoagulants used are also different for each method.
Cellular components
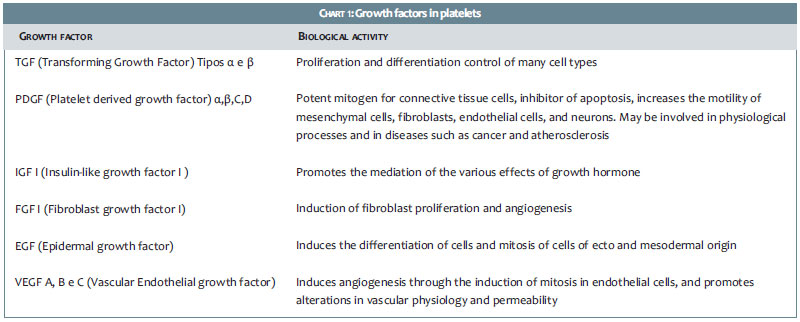
Platelets are anucleated fragments of megakaryocytes, and are produced in the bone marrow.11 They contain granules consisting of various substances, which are released upon activation of the platelets.12 Among the main substances that are released are growth factors (Chart 1), cytokines, adhesion molecules, integrins, and coagulation proteins.
As already mentioned, an important aspect to consider is the amount of erythrocytes and leukocytes in the obtained PRP.
There is disagreement as to the effect caused by leukocytes remaining in the PRP of the treated tissues. Some authors attribute an inflammatory effect-therefore a negative effect-to the presence of white cells in PRP,13 while others attribute antibacterial and immune effects related to the presence of these cells.14 The current perception is that there are significant differences in the biological effects of PRP, according to its cellular content. Dohan et al.15 sought to group different PRP types according to their composition of leukocytes and fibrins. They suggest that the amount of white blood cells present in the PRP has a great influence on the release of growth factors. of the latter. This fact would have an impact on the biological effect of PRP's, entailing difficulties in the comparison and evaluation of clinical results of patients treated with PRP's of different compositions, for instance.
Soluble components
The activation of platelets causes the release of soluble factors present within their granules.12 Platelet activation depends on the adhesion of their surfaces to the molecules present on the damaged endothelium (von Willebrand factor, collagen, fibronectin, and laminin) or occurs through the epinephrine, for instance. It is of paramount importance to note that the molecules present in the endothelium are also expressed in other cell types, as demonstrated by Monteiro:16 the glycoprotein GPIb alpha (present in platelet membranes and exerting the function of mediator of the adhesion to the von Willebrand factor in the vascular endothelium) was also detected in the membrane of dermal cells known as dermal dendrocytes.
The presence of receptors of platelets in the membrane of dermal cells may indicate the participation of these cells in wound healing and repair processes.
It is important to remember that the skin houses different types of stem cells (including cells present in the hair follicle bulge) and cells of mesenchymal origin, all dispersed in the dermis.17 In theory, growth factors released by platelets could act in these cells, promoting differentiation and proliferation. This information should be taken into account when planning to achieve a specific goal with the use of PRP in the skin.
In Table 1 there are descriptions of some of the functions of growth factors released during platelet activation.
Applications in dermatology
The use of PRP in medicine is based on the fact that platelets contain many growth factors in their alpha granules. These factors have a well-known role in the process of tissue repair. Thus, the concentration of these substances in injured tissues could be beneficial to providing more agility to the regeneration processes.
Alopecia
The application of PRP in the treatment of alopecia has been investigated with renewed interest in recent years. Some studies seek to establish the molecular mechanisms through which such patients could benefit from PRP. In an in vitro and in vivo study in animals, Li et al.18 showed that there is a greater proliferation of dermal papilla cells when incubated with PRP, as compared to controls. That effect was due to increased expression of FGF-7 (Fibroblast growth factor 7) and betacatenin, as well as an increase in extracellular signaling of Akt and ERK.
The animals that received subcutaneous injections of PRP had a faster transition from the telogen to the anagen phase as compared to the controls, which received only saline injections. The study by Li et al. indicates the molecular mechanisms through which these results were found, reinforcing the importance of further investigations into the use of PRP for this indication. This study presents LOE 5, given that it is based on physiological mechanisms in animals and cell cultures (Chart 2).
In a study published in 2006, Uebel19 described an apparent improvement in survival rates and take in hair grafts that were exposed to PRP before implantation, as compared to contralateral controls, in a group of 20 male patients. The limitation of this study is linked to the fact that the interpretation of the results was not carried out by independent researchers and also because the area that received the implants treated with PRP was not clearly defined. This study has a LOE 4.
Wound healing
The use of PRP to accelerate the healing of wounds inspires the greatest number of clinical studies. Publications address various issues, such as its use in the treatment of chronic wounds in diabetic patients, in the assessment of the speed of reepithelialization of donor sites in skin grafting, and in the closing of chronic ulcers due to vascular insufficiency, among others.
Two systematic reviews of randomized controlled trials on the use of PRP in the treatment of chronic wounds led to differing conclusions.
After the evaluation of nine clinical trials, Sommeling et al.20 considered that the use of PRP may be beneficial as an adjuvant measure in the treatment of chronic ulcers. Nevertheless, the authors highlight the poor quality of the trials used in the review and the lack of standardization in the methods employed to obtain the PRP and the manner in which it was used.
In a review conducted by Cochrane,21 nine studies were included, totaling 325 treated patients. The authors conducted an analysis of randomized, controlled trials that compared the use of PRP versus a placebo or alternative therapies in the treatment of chronic ulcers (of any etiology) in adults. The studies were selected based on previously defined criteria, such as patient selection, data collection, and risk of bias. After the evaluation of these studies by two independent authors, it was concluded that there was no evidence in favor of the use of PRP in the treatment of ulcers, when compared to placebo or other alternatives. However, due to the small number of studies included in the review, some of them with a risk of bias, the authors suggest that more encompassing and more well-formatted studies were necessary.
According to the Oxford CEBM classification, systematic reviews of randomized controlled trials correspond to LOE 1.
Laser
There are few reports on the association of laser treatments and a concomitant application of PRP. In these studies, a small number of patients underwent treatment with a fractional laser (1,550nm22 and 10,600nm23,24 wavelengths).
In a study by Shin,22 22 patients were treated with a 1,550nm laser, with only half of them receiving topical applications of PRP following the laser sessions. At the end of the study, the group treated with the combination of laser and PRP showed less erythema and greater subjective satisfaction. The authors' conclusion does not suggest a clear superiority of the combined approach as compared to the isolated application of fractional laser.
In two studies23,24 that combine the applications of fractional CO2 laser and PRP (injected intradermally or applied topically after the laser) there was faster recovery of post-laser edema and erythema as well better outcomes (assessed subjectively) when compared to patients who did not receive this treatment.
As with other applications, there was no standardization in the method for obtaining PRP in this case.
These studies are defined as LOE 4.
Rejuvenation
There are few published clinical studies25,26 regarding the use of PRP for rejuvenation purposes, with most of them not clearly describing the method for obtaining PRP, nor clarifying the content of the material obtained. As noted earlier, these data have a fundamental impact on the evaluation of results. Furthermore, many of the studies25 do not have control groups, and others have only photographic images and the subjective impressions of researchers and patients on the final results, as the only method of assessing results. Those studies have LOE 4.
Studies that have used animals27 or cellular cultures28,29 have LOE 5.
The introduction of PRP into the culture medium of human dermal fibroblasts led to an increased proliferation of these cells, as well as to an increased production of collagen,28 in comparison to control cultures that were not incubated with PRP. Likewise, the culture of stem cells derived from adipose tissue in a medium containing PRP also led to the increased proliferation of these cells.29 This finding reinforces the possibility of PRP interfering with the biology of stem cells present in the skin. A similar study carried out in animals showed similar results.26
Annex: Levels of Scientific Evidence
Evidence-based medicine is a concept that unites good scientific research and clinical practice. The practice of this kind of medicine assumes that the choice among therapeutic interventions should be based on the hierarchy of evidence available at the time, among other criteria. This does not mean that the physician's professional experience should not be taken into account, but that good scientific research can help enormously in making therapeutic decisions.
Chart 2 presents a summarized scheme of the LOEs1 proposed by the Oxford Centre for Evidence-Based Medicine, which must be understood in conjunction with the accompanying introductory document2. These LOEs relate solely to issues related to treatment.
The BrazilianMinistry of Health3 adopts this classification in their technical opinions.
1. OCEBM Levels of Evidence Working Group*. "The Oxford 2011 Levels of Evidence". Oxford Centre for Evidence-Based Medicine. http://www.cebm.net/index.aspx?o=5653* OCEBM Table of Evidence Working Group = Jeremy Howick, Iain Chalmers (James Lind Library), Paul Glasziou, Trish Greenhalgh, Carl Heneghan, Alessandro Liberati, Ivan Moschetti,Bob Phillips, Hazel Thornton, Olive Goddard and Mary Hodgkinson
2. Oxford Centre for Evidence-Based Medicine [Internet]. Jeremy Howick, Iain Chalmers, Paul Glasziou, Trish Greenhalgh, Carl Heneghan, Alessandro Liberati, Ivan Moschetti, Bob Phillips, and Hazel Thornton. "The 2011 Oxford CEBM Levels of Evidence (Introductory Document)". [cited 2013 Jul 09]. Available from: http://www.cebm.net/index.aspx?o=5653
3. Ministério da Saúde. Secretaria de Ciência, Tecnologia e Insumos Estratégicos. Departamento de Ciência e Tecnologia. Diretrizes metodológicas: elaboração de pareceres técnico-científicos. 2 ed., rev e ampl. Brasília: Ministério da Saúde; 2009. 62p.
4. Portalmedico.org [Internet]. Brasília: Conselho Federal de Medicina; 2010-2013. Processo-consulta CFM nº 1.477/10 - Parecer CFM nº 20/11. [citado 09 Jul 2013]. Disponível em: http://www.portalmedico.org.br/pareceres/CFM/2011/20_2011.htm
5. Dohan Ehrenfest DM, Rasmusson L, Albrektsson T Classification of platelet concentrates: from pure platelet rich plasma (P-PRP) to leucocyteand platelet rich fibrin (L-PRF). Trends Biotechnol. 2009;27(3):158-67.
6. Guia para o uso de hemocomponentes / Ministério da Saúde, Secretaria de Atenção à Saúde, Departamento de Atenção Especializada. - Brasília: Ministério da Saúde, 2008. 140 p.: il. - (Série A. Normas e Manuais Técnicos)
7. Mazzocca AD, McCarthy MB, Chowaniec DM, Cote MP, Romeo AA, Bradley JP, Arciero RA, Beitzel K. Platelet rich plasma differs according to preparation method and human variability. J Bone Joint Surg Am. 2012 15;94(4):308-16.
8. Boswell SG, Cole BJ, Sundman EA, Karas V, Fortier LA. Platelet rich plasma: a milieu of bioactive factors. Arthroscopy. 2012;28(3):429-39
9. Mazzucco L, Balbo V, Cattana E, Guaschino R, Borzini P. Not every PRPgel is born equal. Evaluation of growth factor availability for tissues through four PRP-gel preparations: Fibrinet, RegenPRP-Kit, Plateltex and one manual procedure. Vox Sang. 2009;97(2):110-8.
10. Dohan Ehrenfest D, Rasmusson L, Albrektsson T. Classification of platelet concentrates:from pure platelet-rich plasma (P-PRP)to leucocyteand platelet-rich fibrin(L-PRF). Trends in Biotechnol. 2009; 27(3):158-67.
11. JWright JH. "The origin and nature of blood plates". Boston Med Surg Journal. 1906;154:643-5.
12. Weyrich AS, Schwertz H, Kraiss LW, Zimmerman GA. Protein synthesis by platelets: historical and new perspectives. J Thromb Haemost. 2009;7(2):241-6.
13. Tidball JG. Inflammatory cell response to acute muscle injury. Med Sci Sports Exerc. 1995;27(7):1022-32.
14. Moojen DJ, Everts PA, Schure RM, Overdevest EP, van Zundert A, Knape JT, et al. Antimicrobial activity of platelet-leukocyte gel against Staphylococcus aureus. J Orthop Res. 2008;26(3):404-10.
15. Dohan Ehrenfest DM, Bielecki T, Jimbo R, Barbé G, Del Corso M, Inchingolo F, et al. the fibrin architecture and leukocyte content influence the growth factor release of platelet concentrates? An evidence- based answer comparing a pure platelet rich plasma (P-PRP) gel and a leukocyte- and platelet rich fibrin (L-PRF). Curr Pharm Biotechnol. 2012;13(7):1145-52.
16. Monteiro MR, Shapiro SS, Takafuta T, Menezes DW, Murphy GF. Von Willebrand factor receptor GPIb alpha is expressed by human factor XIIIa-positive dermal dendrocytes and is upregulated by mast cell degranulation. J Invest Dermatol. 1999;113(2):272-6.
17. Monteiro MR. Células tronco na pele. Surg Cosmet Dermatol 2012;4(2):159-63.
18. Li ZJ, Choi HI, Choi DK, Sohn KC, Im M, Seo YJ, Lee YH, Lee JH, Lee Y. Autologous platelet rich plasma: a potential therapeutic tool for promoting hair growth. Dermatol Surg. 2012;38(7 Pt 1):1040-6.
19. Uebel CO, da Silva JB, Cantarelli D, Martins P. The role of platelet plasma growth factors in male pattern baldness surgery. Plast Reconstr Surg. 2006;118(6):1458-66.
20. Sommeling CE, Heyneman A, Hoeksema H, Verbelen J, Stillaert FB, Monstrey S. The use of platelet rich plasma in plastic surgery: A systematic review. J Plast Reconstr Aesthet Surg. 2013;66(3):301-11.
21. Martinez-Zapata MJ, Martí-Carvajal AJ, Solà I, Expósito JA, Bolíbar I, Rodríguez L, Garcia J. Autologous platelet rich plasma for treating chronic wounds. Cochrane Database Syst Rev. 2012:CD006899.
22. Shin MK, Lee JH, Lee SJ, Kim NI. Platelet rich plasma Combined with Fractional Laser Therapy for Skin Rejuvenation. Dermatol Surg. 2012;38(4):623-30.
23. Na JI, Choi JW, Choi HR, Jeong JB, Park KC, Youn SW, et al. Rapid healing and reduced erythema following ablative fractional CO2 laser resurfacing combined with the application of autologous platelet-rich plasma. Dermatol Surg. 2011;37(4):463-8.
24. Lee JW, Kim BJ, Kim MN, Mun SK. The efficacy of autologous platelet rich plasma combined with ablative carbon dioxide fractional resurfacing for acne scars: a simultaneous split-face trial. Dermatol Surg. 2011;37(7):931-8.
25. Redaelli A, Romano D, Marcianó A Face and neck revitalization with platelet rich plasma (PRP): clinical outcome in a series of 23 consecutively treated patients. J Drugs Dermatol. 2010;9(5):466-72.
26. Kim IS, Park KY, Kim BJ, Kim MN, Kim CW, Kim SE. Efficacy of intradermal radiofrequency combined with autologous platelet rich plasma in striae distensae: a pilot study. Int J Dermatol. 2012;51(10):1253-8.
27. Cho JM, Lee YH, Baek RM, Lee SW. Effect of platelet rich plasma on ultraviolet b-induced skin wrinkles in nude mice. J Plast Reconstr Aesthet Surg. 2011 Feb;64(2):e31-9.
28. Kim DH, Je YJ, Kim CD, Lee YH, Seo YJ, Lee JH, Lee Y.Can Platelet rich plasma be used for skin rejuvenation? Evaluation of Effects of Platelet rich plasma on Human Dermal Fibroblast. Ann Dermatol. 2011;23(4):424-31.
29. Kakudo N, Minakata T, Mitsui T, Kushida S, Notodihardjo FZ, Kusumoto K. Proliferation-promoting effect of platelet rich plasma on human adipose- derived stem cells and human dermal fibroblasts. Plast Reconstr Surg. 2008;122(5):1352-60.
 All content the journal, except where identified, is under a Creative Commons Attribution-NonCommercial 4.0 International license - ISSN-e 1984-8773
All content the journal, except where identified, is under a Creative Commons Attribution-NonCommercial 4.0 International license - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}