


Fred Bernardes Filho1, Maria Victória Quaresma1, Karoline Silva Paolini1, Natalia de Carvalho Rocha1, Bernard Kawa Kac1, Luna Azulay-Abulafia1
Keywords: BLOOD STAINS, NEVI AND MELANOMAS, FOOT
Talon noir is a dermatosis that presents with an asymptomatic petechial lesion, trauma-related and mostly found in acral body sites. It is histologically characterized by blood within the stratum corneum.1 Since its initial description, it has been referred to by several names (Chart 1), with the lesion's description primarily relating to the affected body site and provocative factor2.
The most typical appearance of this clinical entity is the presence of coalescing macules forming a blackened purpuric plaque. It was precisely this appearance that gave rise to the denomination of the dermatosis, termed by the French dermatologist Peachey as talon noir, which means black heel.3 Its pathogenesis is of traumatic origin, and the lesion is caused by excessive tangential pressure applied to the skin. Although it is characteristically bilateral and located in the heels, it can be found on any acral surface.4,5
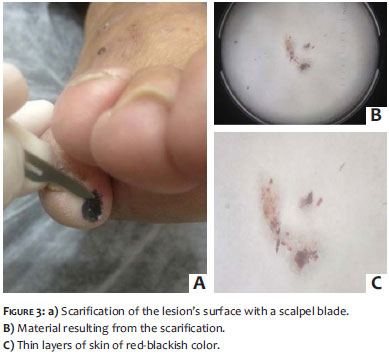
Scarification of the lesion with a scalpel blade allows the detachment of thin layers of pigmented skin that can be evaluated with the aid of dermoscopy or sent for histologic analysis.1 Carrying out a dermoscopy of the lesion is another valuable tool in the diagnosis, for it offers findings that suggest the presence of blood in the stratum corneum.6,7 Diagnostic confirmation is given by the histopathology, which may reveal hyperkeratosis, presence of blood in the stratum corneum and extravasated erythrocytes in the papillarydermis.1
The main differential diagnosis is the presence of melanocytic proliferation, with melanoma being the most important clinical differential diagnosis.1,6 Close inspection is crucial for ruling out simultaneous melanocytic tumor. No treatment is necessary, for the lesions tend to disappear spontaneously.1,2
The present case report is aimed at demonstrating the clinical, dermoscopic, and histopathologic features of this condition, and issuing an alert regarding the importance of including it in the differential diagnosis of lesions that occur in the relevant topography.
A 65-year-old male patient sought the dermatology ambulatory due to the exacerbation of psoriasis lesions and for being off treatment for two years. For roughly two weeks he had had an asymptomatic blackened macular lesion in the fifth right toe, referring no recollection of local trauma.
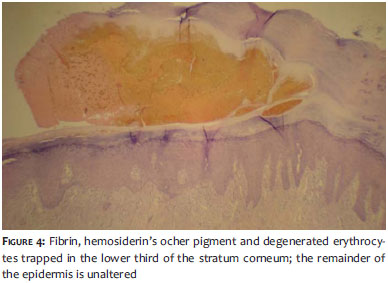
Ectoscopic examination evidenced psoriasiform plaques on the trunk, dorsum, and limbs. The patient had a single red-blackish macula in the medial region of the distal phalanx of the fifth right toe (Figure 1). Dermoscopic analysis verified a homogeneous global pattern with red-blackish color pigment, with the presence of hemorrage minute punctate macules in the periphery (Figure 2). The following hypotheses have been suggested: talon noir and atypical nevus. Scarification of the macula was carried out, resulting in the detachment of blackish colored skin layers (Figure 3). A biopsy of the lesion was performed in order to confirm the diagnosis, and histology revealed fibrin, hemosiderin's ocher pigment, and degenerated erythrocytes trapped in the lower third of the stratum corneum. The remainder of the epidermis had no alteration (Figure 4).
Thus, associating the clinical aspect to the scarification related, dermoscopic, and histopathologic findings, a diagnosis of talon noir was established. The authors instructed the patient about the benign nature of the picture and in the six-week return visit, verified the spontaneous disappearance of the lesion.
Dermoscopy increasingly gains more importance in the clinical practice, with an increasing number of indications.8 This diagnostic method allows the physician to recognize the morphological structures of pigmented skin lesions that can determine whether their nature is melanocytic or not, adding a new dimension to the clinical examination.7,9
In the dermoscopy, the pigmentation seen in lesions in which there is subcorneal hematoma usually has a slightly lighter appearance, revealing a reddish hue. Most often, the overall pattern observed is homogeneous or globular, nevertheless in some cases the pigment may be distributed along the crests, lending a parallel aspect, which makes it even more difficult to differentiate the lesion from acral melanoma.7 In the present case, in addition to the already described dermoscopic features, the authors verified the presence of peripheral hemorrhagic punctate macules.
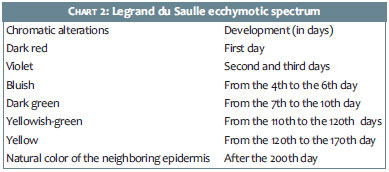
In some cases, the lesion's color may provide clues to their timing and development. The extravasated blood will be reabsorbed, causing chromatic variation from the outset of the condition to the full recovery of the lesion. This variation in hue is known as the Legrand du Saulle ecchymotic spectrum (see Chart 2) and has an important value in forensic traumatology.10 Due to anatomical peculiarities, some body sites such as the ocular conjunctiva, fingers, and palmoplantar regions do not present ecchymotic spectrum.10
The authors propose that in the presence of dermoscopic findings suggestive of subcorneal hematoma in a patient who presented local trauma, an expectant approach can be taken for 30 days to evaluate the development. The occurrence of spontaneous regression is consistent with the diagnosis of talon noir. In the present case, by considering the hypothesis of melanocytic lesion, and due to the fact that the patient did not remember having had a trauma in the relevant site, the authors chose to perform an incisional biopsy for diagnostic confirmation.
The authors emphasize the importance of adding talon noir to the differential diagnosis of melanocytic lesions, including melanoma, and suggest the use of dermoscopy as an auxiliary method in the diagnosis.
1. Urbina F, Leon L, Sudy E. Black heel, talon noir or calcaneal petechiae? Australas J Dermatol. 2008;49(3):148-51.
2. Tlougan BE, Mancini AJ, Mandell JÁ, Sanchez MR. Skin conditions in figure skaters, ice-hockey players and speed skaters: part I - mechanical dermatoses. Sports Med. 2011;41(9):709-19.
3. Crissey JT, Peachey JC. Calcaneal petechiae. Arch Dermatol. 1961;83:501.
4. Yaffee H. Talon noir. Arch Dermatol. 1971;104(4):452.
5. De Luca JF, Adams BB, Yosipovitch G. Skin manifestations of athletes competing in the summer olympics: what a sports medicine physician should know. Sports Med. 2012 1;42(5):399-413.
6. Rubegni P, Feci L, Fimiani M. Talon Noir: utility of dermoscopy for differential diagnosis with respect to other acral skin growths. G Ital Dermatol Venereol. 2012;147(1):133-4.
7. Ferreira CMM, Barcaui C, Piñeiro-Maceira J. Outras dermatoses de interesse dermatoscópico. In: Atlas de Dermatoscopia. Aplicação clínica e correlação histopatológica. Rio de Janeiro: DiLivros; 2011. p. 189-98.
8. Bastos CAS. Non-traditional Indications in dermoscopy. Surg Cosmet Dermatol. 2012;4(2)203-5.
9. Rezze GG, Sá BCS, Neves RI. Dermatoscopia: o método de análise de padrões. An Bras Dermatol. 2006;81(3):261-8.
10. Periciamedicalegal. com. br [Internet]. Perícia Médica Legal. Importância forense do espectro equimótico [acesso 08 Abr 2013]. Disponível em: http://periciamedicalegal.com.br/?p=6.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}