


Emerson Henrique Padoveze1, Selma Schuatz Cernea1
Keywords: MOHS SURGERY, CARCINOMA, BASAL CELL, CARCINOMA, SQUAMOUS CELL
Skin tumors are the most common neoplasm in humans. The estimated incidence of non-melanoma skin cancer in Brazil for 2013 is 134,000 new cases-62,680 in men and 71,490 in women. These values correspond to the estimated risk of 65 to 71 new cases per 100,000 men and women, respectively.1
Basal cell carcinoma (BCC) is the most common type and accounts for approximately 75% of these lesions, followed by the squamous cell carcinoma (SCC) with an incidence of 15% and, more rarely, by melanoma, which in Brazil corresponds to 4% of cutaneous malignancies.2,3 The most common site of occurrence is on the face, with 70% located on the nose and forehead.
The Mohs micrographic surgery technique (MMS) is used to perform the mapping of 100% of the margins, allowing the complete removal of the lesion, which translates into high cure rates. The five-year recurrence rate of primary and recurrent BCC treated with conventional surgery is 10% and 17%, respectively. In tumors treated with MMS that rate decreases to 1% and 6%.4 The MMS technique also spares normal tissue, which results in smaller surgical wounds.5
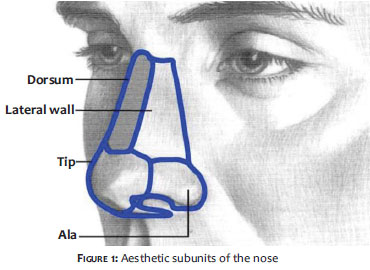
The complex contours of the nose reflect the different structures by which it is formed, as well as the different features of the skin that covers it. While the skin is thick and sebaceous in the nasal tip and wings, it is thin in the dorsum and lateral regions. In addition, the skin has greater mobility in the upper two-thirds of the nose. The combination of these factors leads to the creation of aesthetic subunits of the nose (dorsum, tip, lateral wall, nasal ala, and columella) (Figure 1).6 The reconstruction of surgical defects generated by the excision of tumors on the nose is a challenge for dermatologic surgeons, due to its rigid structure and limited mobility.
In the reconstruction of nasal defects, the fulfillment of some basic principles is essential for a good aesthetic result. Initially, it is necessary to determine the surgical wound's characteristics (topography, length, and depth). When possible, the limited availability of tissue at the site should be offset by the best available equivalent, which in the nose region is the skin adjacent to the wound. Another principle that must be followed is to respect the aesthetic units, aiming at locating scars in the natural folds and furrows of the nose.7 In cases where the tumor affects more than 50% of an aesthetic unit, some authors recommend the complete excision of the subunit, closing the wound with an advancement flap or graft to minimize tissue contrasts.8,9
Many techniques can be used in the closure of surgical defects that result from the excision of tumors on the nose, among them are the side-to-side closure, the advancement flap, the transposition flap, the bilobed flap, grafts or a combination of techniques.
The objective of the present study is to demonstrate the available techniques for correcting surgical defects on the nose, according to the anatomical location of the tumor, in patients who underwent CMM at the Dermatology Service of the Hospital do Servidor Público Municipal de São Paulo (HSPM), (SP) Brazil, between 1996-2010.
A descriptive study of patients who underwent CMM at the Dermatology Service of the HSPM during the years 1996-2010 was carried out. Medical records and pre-, intra-, and post-operative photographs of patients who underwent exeresis of tumors in the nasal region were analyzed in order to correlate the surgical defect's anatomical location and the type of reconstruction to be adopted. The study excluded patients whose lesions extended into more than one nasal sub-unit or the limits of the nose, as well as those who did not have a complete photographic record.
Two hundred and thirty-six (236) patients were operated on, with 279 tumors removed from the nasal region through CMM during the 1996-2010period. Of these patients, 170 were included in the study (109 women and 61 men, with a total of 203 lesions). The patients' ages ranged from 19-93 years (mean = 65 years).
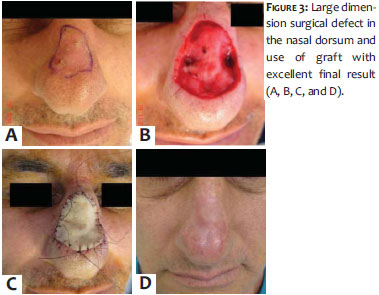
Treated neoplasms corresponded to 190 BCCs and 13 SCCs. The following distributions were verified, according to the anatomical location: 68 lesions in the nasal alae, 62 in the nasal dorsum, 40 on the nasal tip, and 33 in the lateral wall of the nose (Graph 1).
The following techniques were used for reconstruction of defects in the nasal dorsum: 18 grafts, 17 advancement flaps, 13 direct sutures, 7 bilobed flaps, and 5 transposition flaps. Combined techniques (direct suture and graft or advancement flap and graft) were performed in 2 patients.
In lesions on the nasal tip, 16 cases were closed with grafts, 9 with bilobed flaps, 8 with advancement flaps, 6 with direct sutures, and 1 with transposition flap.
For lesions located in the lateral wall, the advancement flap was used more often (16 cases), followed by the bilobed flap (7 cases), direct suture (six cases), graft (2 cases), transposition flap (1 case) and a combination of advancement and transposition flap (1 case).
Finally, of the 68 surgical defects located in the nasal ala, 33 were reconstructed with advancement flaps, 17 with transposition flaps, 8 with bilobed flaps, 5with grafts, 4 with direct sutures, and 1 with the combination of transposition flap and graft.
The distribution of the surgical techniques used for closure of the lesions according to the anatomical location of the surgical defect is depicted in the pie charts of Graph 2.
The closure of nasal defects is often difficult when it comes to achieving good functional and aesthetic outcomes. The patient's age, and size and location of the surgical defect are the parameters that guide the choice of the best reconstruction method.
MMS is considered the most reliable method to approach skin cancer for it allows the histologic control of the margins of excised tumors, resulting in cure rates that exceed those of other therapeutic modalities, in addition to providing the maximum conservation of healthy tissue.4 Nevertheless, there are several challenges regarding the reconstruction of the nose in day-to-day practice.
In the present study, it was possible to observe that the topographical location of the most common tumors of the nose was the nasal ala (33% of cases), followed by the dorsum (30%). This data is consistent with the literature, which states that most tumors of the nose are located in the distal two thirds.8,9 Brata et al. studied 1,131 patients who underwent MMS and verified that the most common sites of neoplastic involvement were the nasal alae and dorsum.10
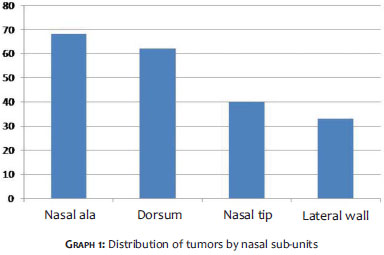
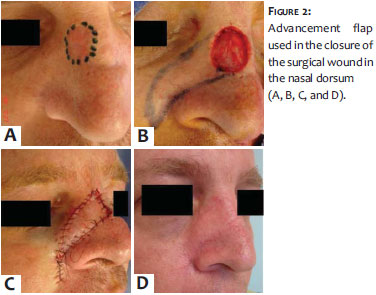
In the nasal dorsum, grafts (29% of cases) and advancement flaps (28%) were the most frequently used techniques for correcting surgical defects (Figures 2 and 3). Since the skin of the dorsum of the nose is thin and very mobile, flaps in this region should always be considered, unless there is fibrosis linked to prior surgeries that may preclude its mobility.11 In such cases-or in large surgical wounds-grafts become the best option due to being thinner, and the number of sebaceous glands in that region.8,12
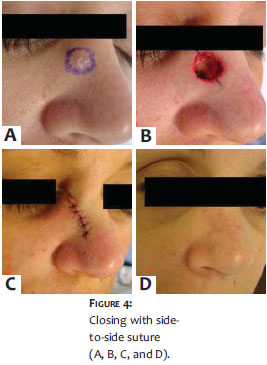
In addition to these two types of reconstruction, the side-to-side closure (21% of cases) was widely used in defects in the nasal dorsum of the present study's patients. A fundamental principle governing reconstructive surgery is that the simplest route must be always chosen, meaning primary closure is the best option whenever it can be attained (Figure 4).13 Nonetheless, the relative number of such procedures was lower than that for flaps and grafts, evidencing the number of moderate to large surgical defects present in the study's sample.
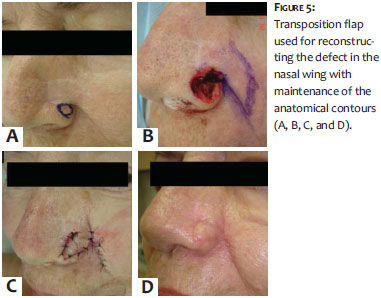
For lesions located in the nasal alae, the greatest challenge is to maintain the natural curvature of the nose without flattening it, keeping the respiratory function and intact balance with the opposite side.14 Of such defects, 49% were reconstructed with alar advancement flaps, 25% with nasogenian transposition flaps, and 12% with bilobed flaps. This data is consistent with the literature. Half of the study's patients bearing lesions in that subunit (nasal alae) had relatively small lesions located below the nasal sulcus, allowing for the performing of alar flaps. Bilobed flaps are often used for the reconstruction of the dorsum and of the inferolateral third of the nose.15 Nasogenian flaps are widely used for repairs in the nasal tip and alae due to their good blood supply and the availability of redundant skin, offering good conditions for reconstruction.16 The transposition flap is a good option for lesions located close to the nasal alae's free margins because it does not raise the nostril and provides for the rebuilding of the nasal ala (Figure 5).17
Twenty-four of the 33 lesions (72%) which affected the side wall of the nose were closed with flaps-of which the most used was the advancement flap, corresponding to 49% of cases (Figure 6). The literature quotes advancement flaps from the jugal region to repair defects in the nasal lateral wall and dorsum due to their high mobility capacity.18
Regarding the tip of the nose, the techniques used more often in these cases were: grafts (40% of cases), bilobed flaps (22%), advancement flaps (20%), and direct suture (15%). It is important to note that for smaller lesions bilobed and advancement flaps were the most successful, resulting in excellent final results (Figure 7). In fact, some authors consider bilobed flaps, as well as the primary closure, very efficient for small defects of the nasal tip.19 For larger lesions, grafts have proven a good option as there was no deviation of the nose. Another possibility reported in the literature for the reconstruction of large defects in the nasal tip includes the frontal flap, however this technique was not included in the present study due to the exclusion of cases in which the wound exceeds more than one nasal sub-unit, or the limits of the nose. Furthermore, this reconstruction type requires a second surgical visit for the resection of the pedicle.
In the present study, it was observed that most of the grafts was performed in the early years of the analyzed period and that, as more experience and surgical skill were accumulated by surgeons of the dermatologic service, flaps were included in the preferred techniques for reconstructing large defects in the nose. According to the literature, this concept of restorative surgery-which prioritizes flaps over grafts whenever possible-developed in other dermatologic services worldwide due to the fact that the use of skin from the same aesthetic unit provides perfect texture and color.8,20
The dermatologic surgeon must bear in mind the principle that when choosing the most appropriate method, the reconstruction must be as simple as possible and based on their technical capacity, and should also take into consideration the characteristics of each patient.
1. Instituto Nacional de Câncer José Alencar Gomes da Silva. Estimativa 2012 : incidência de câncer no Brasil. [Internet]. Rio de Janeiro: Inca; 2011 [citado 17 Jun 2013]. Disponível em: http://www.inca.gov.br/estimativa/2012/estimativa20122111.pdf
2. Enokihara MY, Simões MM, Enokihara S. Carcinoma Basocelular e Carcinoma Espinocelular. In: Lupi O, Belo J, Cunha PR, editores. Rotinas de Diagnóstico e Tratamento da Sociedade Brasileira de Dermatologia. São Paulo: AC Farmacêutica; 2010. p. 29-35.
3. Miller SJ. Biology of basal cell carcinoma (Part 1). J Am Acad Dermatol. 1991;24(1):1-13.
4. Reis NA, Azevedo LCM, Stolf HO, Nouri K, Kimyai-Asadi A, Goldberg LH. Cirurgia micrográfica de Mohs. Surg Cosmet Dermatol. 2011;3(3):227-31.
5. Terzian LR, Nogueira VMA, Paschoal FM. Cirurgia Micrográfica de Mohs para preservação tecidual nas cirurgias oncológicas da face. Surg Cosmet Dermatol. 2010;2(4):257-63.
6. Larrabee FWJr, Sherris DA. Principles of Facial Recontruction. Philadelphia: Lippincott; Williams & Wilkins; 1995.
7. Smadja J. Crescentic Nasojugal Flap for Nasal Tip Reconstruction. Dermatol Surg. 2007;33(1):76-81.
8. Beer GM, Bermoser K, Kompatscher P. Closure of Nasal Defects After Tumor Excision with Local Flaps. Aesthetic Plast Surg. 1998;22(1):42-7.
9. Van der Eerden PA, Verdam FJ, Dennis SC, Vuyk H. Free cartilage grafts and healing by secondary intention: a viable reconstructive combination after excision of nonmelanoma skin cancer in the nasal alar region. Arch Facial Plast Surg. 2009;11(1):18-23.
10. Batra RS, Kelley LC. Predictors of Extensive Subclinical Spread in Nonmelanoma Skin Cancer Treated With Mohs Micrographic Surgery. Arch Dermatol. 2002;138(8):1043-51.
11. Iida N, Ohsumi N, Tonegawa M, Tsutsumi K. Repair of Full Thickness Defect of the Nose Using an Expanded Forehead Flap and a Glabellar Flap. Aesthetic Plast Surg. 2001;25(1):15-9.
12. Wee SS, Hruza GJ, Mustoe TA. The frontonasal flap: utility for lateral nasal defects and technical refinements. Br J Plast Surg. 1991;44(3):201-5.
13. Wesley NO,Yu SS, Grekin RC, Neuhaus IM. Primary linear closure for large defects of the nasal supratip. Dermatol Surg. 2008;34(3):380-4.
14. Uchinuma E, Matsui K, Shimakura Y, Murashita K, Shioya N. Evaluation of the Median Forehead Flap and the Nasolabial Flap in Nasal Reconstruction. Aesthetic Plast Surg. 1997;21(2):86-9.
15. Fujiwara M. One-stage reconstruction of an alar defect using a bilobed nasolabial-nasal tip flap based on the aesthetic subunits in Orientals: case report. Aesthetic Plast Surg. 2004;28(1):13-6.
16. Turan A, Kul Z,Turkaslan T, Ozyigit T,Ozsoy Z. Reconstruction of lower half defects of the nose with the lateral nasal artery pedicle nasolabial island flap. Plast Reconstr Surg. 2007;119(6):1767-72.
17. Van der Eerden P, Simmons M, Vuyk H. Reconstruction of Nasal Sidewall Defects After Excision of Nonmelanoma Skin Cancer. Analysis of Uncovered Subcutaneous Hinge Flaps Allowed to Heal by Secondary Intention. Arch Facial Plast Surg. 2008;10(2):131-6.
18. Chen EH, Johnson TM, Ratner D. Introduction to flap movement: reconstruction of five similar nasal defects using different flaps. Dermatol Surg. 2005;31(8 Pt 2):982-5.
19. Belmahi A, El Mazouz S, Gharib NE, Bencheikh R, Ouazzani S. The bilobed flap: a very efficient method in aesthetic reconstruction of small skin defects at the alar and tip regions of the nose. Ann Chir Plast Esthet. 2003;48(4):211-5.
20. Weber SM, Baker SR. Management of cutaneous nasal defects. Facial Plast Surg Clin North Am. 2009;17(3):395-417.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}