


Emerson Vasconcelos de Andrade Lima1, Mariana de Andrade Lima1, Daniela Takano1
Keywords: DESEARCH DESIGN, COLLAGEN, WOUND HEALING, AMBULATORY SURGICAL PROCEDURES, REJUVENATION
The proposal to use ablative treatments aimed at stimulating and remodeling collagen has long been advocated in the field of dermatology. It is widely known that the mechanical or chemical removal of the epidermis triggers the release of cytokines and the migration of inflammatory cells, resulting in the replacement of damaged tissue by cicatricial tissue.1 Medium and deep chemical peels are examples of ablative treatments that are popular among dermatologists due to their indisputable stimulation of collagen production, which results in the attenuation of wrinkles, improvement of texture, brightness and color of the cutaneous surface, in addition to their capacity for correcting depressed scars, and relieving photodamage.2 However, the recovery for these procedures is protracted and results in sensitive tissue that is subject to post-inflammatory hyperpigmentation and photosensitivity, in addition to the risk of complications such as hypertrophic scarring, persistent erythema, and dyschromias. Currently, a trend is being observed towards the indication of less invasive procedures, isolated or in conjunction, aimed at reducing the risk of complications and allowing a patient's earlier return to normal life. The microneedling principle proposes a stimulus for the production of collagen, without causing the total de-epithelization observed in ablative techniques.
Microneedling fundamentals
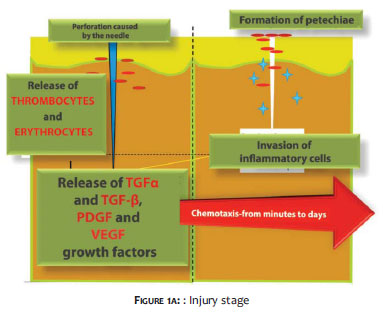
Orentreich and Orentreith3 were the first to describe the use of needles aimed at stimulating collagen production in the treatment of depressed scars and wrinkles, a technique that became known by the term subcision. Based on the same principle of rupturing and removing damaged subepidermic collagen and subsequently replacing it with new collagen and elastin fibers, other authors confirmed this initial study.4 More recently there has been a proposal for a system of microneedles that is applied to the skin with the objective of generating multiple micropunctures, which are long enough to reach the dermis and cause bleeding, triggering inflammatory stimuli that results in the production of collagen.5 The percutaneous collagen induction (PCI), as the technique has been called, begins with the cutaneous barrier loosing its integrity (aimed at dissociating keratinocytes), resulting in the release of cytokines such as interleukin-1α (predominantly), interleukin-8, interleukin-6,TNF-α and GM-CSF, and leading to dermal vasodilation and migration of keratinocytes, a process that restores the epidermal damage.6 For didactic purposes, three stages of healing following trauma with needles can be clearly delineated: in the first stage (injury stage) is a release of platelets and neutrophils (which are responsible for releasing growth factors that act on keratinocytes and fibroblasts as growth and transformation factors α and β (TGFα and TGF-β), of platelet-derived growth factor (PDGF), of Protein III (activator of connective tissue), and connective tissue growth factor (Figure 1A).
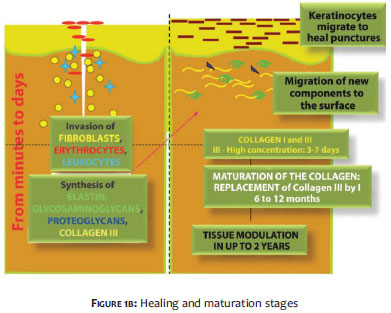
In the second stage (healing stage), neutrophils are replaced by monocytes and angiogenesis, epithelialization and fibroblast proliferation take place, followed by the production of type III collagen, elastin, glycosaminoglycans and proteoglycans. Concomitantly, fibroblasts growth factor,TGFα and TGF-β are secreted by monocytes. Roughly five days after the injury inflicted, the fibronectin matrix is completely formed, allowing the deposition of collagen directly beneath the basal layer of the epidermis (Figure 1B).
In the third stage (maturation stage), type III collagen, which is prevalent in the early phase of the healing process is slowly replaced by type I collagen (which lasts longer and persists for a period ranging from five to seven years).7-9 In order for this inflammatory sequence of events to take place, the trauma caused by the needle must reach a depth of 1-3mm, and the epidermis must be preserved (only perforated and not removed).5 Hundreds of microlesions are created, resulting in columns of blood collected in the dermis, accompanied by edema of the treated area and virtually immediate hemostasis. The intensity of these reactions is proportional to the length of the needle used in the procedure.
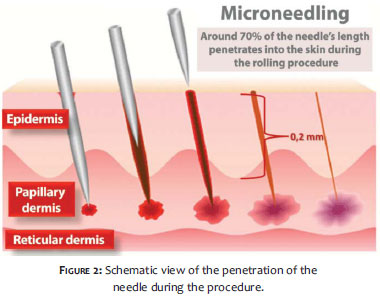
For instance, a1mm depth entails an almost microscopic hematoma, while that resulting from a 3mm depth can be seen with the naked eye and can persist for hours. Nonetheless, it is necessary to understand that the needle does not penetrate completely during the rolling process (Figure 2).
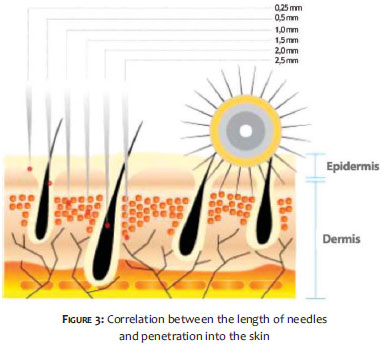
It is estimated that a 3mm long needle penetrates only 1. 5-2mm (or roughly 50-70% of its total length). Therefore, with a 1mm long needle the injury caused to the skin would be limited to the superficial dermis, resulting in a more limited inflammatory response than that caused by a longer needle (Figure 3).
Characteristics of the microneedling technique
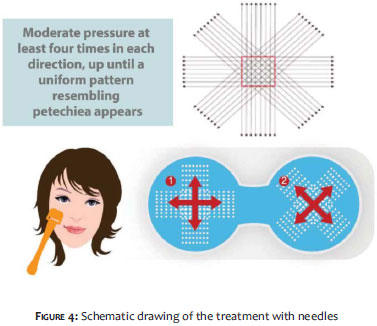
The device used to perform microneedling comprises a polyethylene roll studded with sterile stainless steel needles symmetrically aligned in rows, with a total of 190 units on average (a number that may vary depending on the manufacturer). The length of the needles is fixed throughout the structure of the roll and varies from 0. 25-2. 5 mm, according to the model. The procedure is usually well tolerated under local anesthesia, with needles not exceeding 1mm in length. For greater lengths, anesthetic blockade supplemented by infiltrative anesthesia is recommended. With the aim of providing more comfort for the patient in situations of a prolonged surgical time and deeper injury, local anesthesia with sedation is recommended. Microneedling is a technique-dependent procedure and familiarization with the device used and mastery of the technique are factors that directly influence the final outcome.10 The vertical pressure exerted on the roller must not exceed 6N, because greater force can damage deeper anatomical structures and cause excessive pain. It is recommended to position the device between the thumb and index finger-as if holding a Hashi-controlling the force with the thumb. The back and forth movements must imprint a uniform pattern of perforations (resembling petechiae) throughout the treated area. In order to achieve this, 10-15 passes in the same direction must be made, and at least four crossing passes in the rolling areas seem to be sufficient. In theory, 15 passes allow a damage corresponding to 250-300 punctures/cm2 (Figure 4).
The time that the petechiae pattern takes to arise varies according to the thickness of the treated skin and the selected needle's length. Therefore, a thinner and looser skin, which is usually photodamaged, will present a uniform petechiae pattern earlier than a thicker and fibrotic skin, which is commonly observed in patients with acne scars, for example. In this manner, the choice of the needle's length depends on the type of the skin to be treated and the ultimate goal of the procedure. There is not yet a classification correlating the length of the device's needles to the depth of the expected damage in the treatment.
The present study's proposal is to establish the correlation between the length of the needle used, to the depth of the resulting damage, using in this first stage of research the skin of living pigs, considering it as the model that is most similar to human skin.
Dr. Roller® devices (Moohan Enterprise Co. , Gyeonggi-Do, South Korea), duly registered with ANVISA, the Brazilian Health Surveillance Agency (under the number 80669600001), composed of 192 stainless steel needles, arranged in eight rows across the extension of a polyethylene roller, sterilized with gamma rays, were used in the experiment. The investigation was performed in vivo, on the skin of live pigs. The pigs underwent general anesthesia and were kept under assisted respiration in the Experimental Surgery Laboratory of the Universidade de São Paulo. The experiment was approved by the Research Ethics Committee.
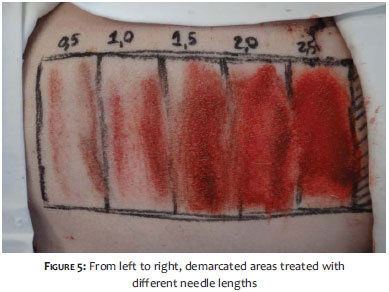
The animal's dorsum's right side region was divided into tracks on which the roller with needles was passed back and forth, for two or three minutes. Rollers with needles measuring 0. 5mm, 1mm, 1. 5mm, 2mm and 2. 5mm in length were used (Figure 5). Immediately after the procedure, a sample of each area was collected using a scalpel blade n. 11, formolized and sent for histologic analysis. After undergoing the hystologic processes, specimens were micro-cut into 5µ sized specimens, which were stained with hematoxylin and eosin, and subsequently evaluated through optical microscopy.
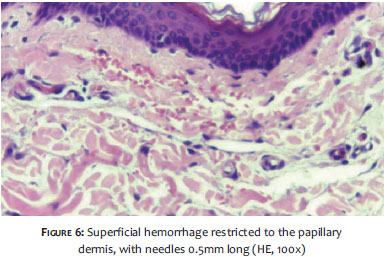
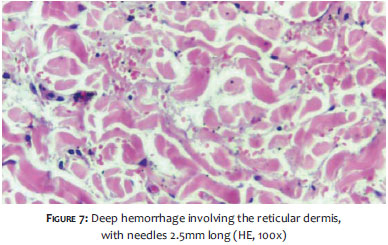
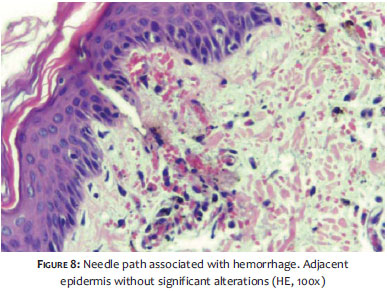
The macroscopic appearance of the pigs' skin after treatment (Figure 5) evidently suggests that the damage caused by the microneedling holds a proportional relation to the length of the needle used. The microscopic examination in the first stage (immediately after the injury) revealed predominantly vascular ectasia with the extravasation of erythrocytes. This finding was observed superficially, having affected the papillary dermis with 0. 5mm needles (Figure 6), reaching the reticular dermis with needles of greater length (Figure 7). The amount of bleeding was also increased proportionally to the length of the needles. The epidermis remained apparently intact under optical microscopy, except for the presence of the needle path site (Figure 8). None of the samples presented lesions in the subcutaneous tissue.
Classification of the severity of the injury caused by microneedling
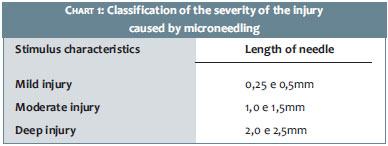
Based on the results, the authors propose the classification of the injury as mild, moderate and deep, correlating to the needles' length and their ability to induce the planned trauma (Table 1).
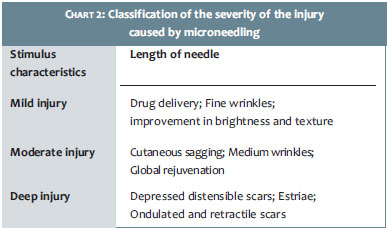
Further, the authors also propose a correspondence between the type of injury and the most appropriate indications, described in Table 2.
In this manner, based on the authors' experience and evaluation of the available literature, considerations were made that microneedling can be used:
A) As a delivery system for active principles in rejuvenation, such as retinol and vitamin C.
B) As an isolated stimulus in the rejuvenation of the face, improving color, texture, and brightness of the skin.
C) In the treatment of sagging skin and the attenuation of wrinkles, given that it promotes the production of collagen, and provides increased volume in the treated area, based on the stimulus described in item B.
D) In the correction of distensible, depressed, corrugated, and retractile scars, as well as in the improvement of old and recent stretch marks.
Advantages of microneedling
• The procedure allows the stimulation of collagen production without removing the epidermis.
• The healing time is shorter and the risk of side effects is reduced as compared to ablative techniques.
• The skin becomes thicker and more resistant, unlike in ablation techniques, where the cicatricial tissue is more susceptible to photodamage.
• It is indicated for all skin types and colors, and can also be used in areas of a lower concentration of sebaceous glands.
• Low cost when compared to procedures that require technologies demanding high investment values.
Disadvantages of microneedling
• It is a technique-dependent procedure and requires training.
• Requires prolonged recovery time if moderate to deep injury are indicated.
• Demands careful assessment of the patient on the part of the physician, and a therapeutic proposal compatible with possible outcomes that can be achieved, avoiding unrealistic expectations.
Microneedling is an innovative treatment that can be used for a broad spectrum of indications when the objective is to stimulate the production of collagen, constituting an additional weapon in the dermatologist's therapeutic armamentarium. The goal of the present study was to establish the correlation between the length of the needle used in the roller and the extent of damage caused to the skin, thereby facilitating the choice of instrument in different indications. The behavior of human skin under the effects of microneedling will be the subject of the authors' next research, nevertheless they believe that the model used in the present study (the skin of live pigs), provides us with answers to questions that had not been addressed by scientific articles to date. The authors believe that the present paper's results will contribute to the proper use of this technique, which has offered a good therapeutic response when properly indicated. It is up to the individual dermatologist to perform an accurate assessment of the lesion to be treated, and to be technically prepared to conduct the procedure within the recommended precepts.
1. Cohen KI, Diegelmann RF, Lindbland WJ. Wound healing: biochemical and clinical aspects. Philadelphia: W. B. Saunders Co; 1992.
2. Brody HJ. Trichloracetic acid application in chemical peeling, operative techniques. Plast Reconstr Surg. 1995;2(2):127-8.
3. Orentreich DS, Orentreich N. Subcutaneous incisionless (subcision) surgery for the correction of depressed scars and wrinkles. Dermatol Surg. 1995;21(6):6543-9.
4. Camirand A, Doucet J. Needle dermabrasion. Aesthetic Plast Surg. 1997;21(1):48-51.
5. Fernandes D. Minimally invasive percutaneous collagen induction. Oral Maxillofac Surg Clin North Am. 2006;17(1):51-63.
6. Bal SM, Caussian J, Pavel S, Bouwstra J A. In vivo assessment of safety of microneedle arrays in human skin. Eur J of Pharm Sci. 2008;35(3):193-202.
7. Fernandes D, Massimo S. Combating photoaging with percutaneuos collagen induction. Clin Dermatol. 2008;26(2):192-9.
8. Aust MC. Percutaneuos Collagen Induction therapy (PCI)-an alternative treatment for scars. Wrinkles Skin Laxity. Plast Reconstr Surg. 2008;121(4):1421-9.
9. Aust MC. Percutaneuos Collagen Induction therapy (PCI)-minimally invasive skin rejuvation with risk of hyperpigmatation- fact or fiction? Plast Reconstr Surg. 2008;122(5):1553-63.
10. Fabroccini G, Fardella N. Acne scar treatment using skin needling. Clin Exp Dermatol. 2009;34(8):874-9.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}