


Flavia Vieira Brandão1; Gisele Gargantini Rezze2; Juliana Machado Canosa3
The prognosis of cutaneous melanomas depends mainly on the lesions' thickness; early detection is of paramount importance for patient longer survival rates. An accuracy of approximately 90% can be achieved using dermoscopic assessment. Since early melanomas might not present specific dermoscopic features, they can only be diagnosed by observing alterations over time through total body mapping and serial digital dermoscopy. Patients with atypical nevus syndrome and multiple familial melanoma presented a higher sensitivity for the detection of melanoma using that technique.
Keywords: MELANOMA; DERMOSCOPY; DYSPLASTIC NEVUS SYNDROME.
The incidence of melanoma has been increasing considerably in recent decades. Although it is the least common of the skin cancers, it is responsible for most deaths. The best treatment is still early diagnosis, with the surgical removal of the primary lesion.1,2 Dermoscopy is a noninvasive method that can aid in the diagnosis of melanoma in early stages. 1, 3
Some melanomas do not show typical characteristics under dermoscopy, with the diagnosis being carried out only by the analysis of the alterations 4 observed over time through serial digital dermoscopy.
The present paper reports the case of 35-year-old, white male patient iving in Sao Paulo, Brazil. The patient's family history included a mother with a history of skin melanoma.
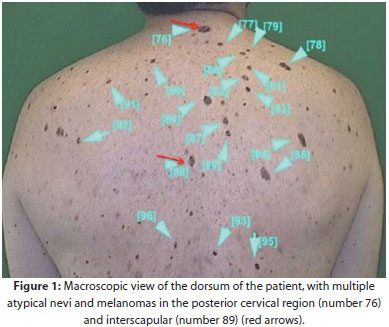
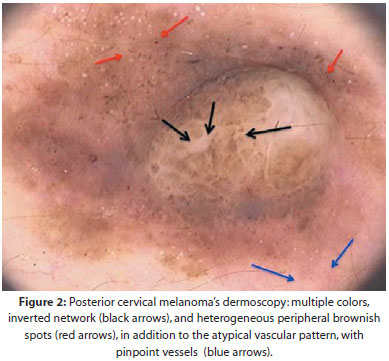
The patient sought care at the Hospital A.C. Camargo in São Paulo (SP), Brazil, to undergo total body mapping and digital dermoscopy in January 2011, due to the family history of melanoma and the presence of multiple common and atypical nevi. In the first examination, 117 lesions were observed, four of them with removal indication (Figure 1). The histologic analysis suggested the presence of three atypical nevi and one melanoma of the superficial spreading type. The latter was located in the posterior cervical region, having been identified as number 76 of the body mapping, with a 0.85 mm Breslow index thickness, a mitotic index of 0/10 high-power fields (HPF), 0mm2, absence of ulceration or regression, and association with compound melanocytic nevus (Figure 2).
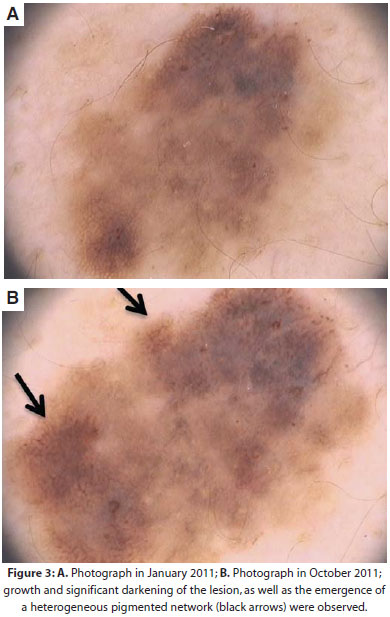
The patient did not return for follow-up treatment, three months later, as instructed. In October 2011, in the second digital dermoscopy – nine months after the first examination – growth and alterations in the pigmentation and pigmented network of three additional lesions were observed, with removal indication. The histhopathological results suggested two atypical nevi and one additional melanoma of the extensive superficial type, the latter identified as number 89 of the body mapping, being located in the interscapular region, with a Breslow thickness of 0.4 mm, mitotic index of 0/10 HPF, 0mm2, absence of ulceration or regression, and association with pre-existent melanocytic nevus (Figures 3A and 3B).
Dermoscopy offers an increase of 10 to 27% in the accuracy in melanoma diagnosis as compared to the naked eye examination, allowing the detection of lesions in early stages and improving patient survival rates.4,5
Nevertheless, early melanomas can be uncharacteristic under dermoscopy in the first examination, only being recognizable through alterations over time.5 The first follow-up visit in digital dermoscopy, three months after the first examination, is of paramount importance for the detection of fast growing melanomas, with any alteration in the size, shape, dermoscopic structures or color that might occur in that monitoring interval being indicative for exeresis.4
The body mapping and digital dermoscopy allow the detection of thinner and incipient melanomas, 3,5 with patients at the most risk of developing melanoma (such as those with atypical nevus syndrome and multiple familial melanoma, similar (to the patient described) benefitting most from that type of examination.3
At the time this article went to press, the patient studied was being followed up, clinically and dermoscopically, at the outpatient clinic of the Núcleo de Câncer de Pele e Dermatologia do Hospital A.C. Camargo (Center for Dermatology and Skin Cancer of the Hospital A.C. Camargo).
1. Braun RP, Rabinovitz HS, Oliviero M, Kopf AW, Saurat JH. Dermoscopy of pigmented skin lesions. J Am Acad Dermatol. 2005; 52(1): 109-21.
2. Shoo BA, Kashani-Sabet M. Melanoma arising in African-, Asian-, Latino- and Native-American populations. Semin Cutan Med Surg. 2009; 28(2):96-102.
3. Haenssle HA, Korpas B, Hansen-Hagge C, Buhl T, Kaune KM, Johnsen S, et al. Selection of patients for long-term surveillance with digital dermoscopy by assessment of melanoma risk factors. Arch Dermatol. 2010;146(3):257-64.
4. Menzies SW, Gutenev A, Avramidis M, Batrac A, McCarthy WH. Shortterm digital surface microscopic monitoring of atypical or changing melanocytic lesions. Arch Dermatol. 2001;137(12):1583-9.
5. Neila J, Soyer HP. Key points in dermoscopy for diagnosis of melanomas, including difficult to diagnose melanomas, on the trunk and extremities. J Dermatol. 2011; 38 (1): 3-9.
This study was carried out at Hospital AC Camargo of the Fundação Antonio Prudente - São Paulo (SP), Brazil.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}