


Alceu Luiz Camargo Villela Berbert1; Sônia Antunes de Oliveira Mantese2; Karen Renata Nakamura Hiraki3; Adriano Mota Loyola4; Naiana Pereira Queiroz5
Summary: Multiple cutaneous miliary osteoma is a rare condition characterized by ectopic bone tissue in the dermis and/or hypodermis. It usually occurs on the face, in individuals of 17 to 79 years old. Its etiology is still unknown. The present article reports the case of a female patient affected by a hardened, poorly delimited, papular plaque of dark brown hue and irregular surface, affecting the malar and mentonian regions. The patient sought medical care two years before the publication of this study, describing untreated acne since the age of 16. The papular plaque was composed of hyperchromic papular nodular lesions – some with white-yellowish hue. The diagnosis was confirmed histopathologically. Satisfactory therapeutic results were achieved with the use of 0.1% tretinoin cream.
Keywords: OSTEOMA; DECALCIFICATION, PATHOLOGIC; OSSIFICATION, HETEROTOPIC.
Multiple cutaneous miliary osteomas (MCMO)is a rare disorder characterized by the presence of ectopic bone tissue in the dermis and/or in the hipodermis.1 It usually occurs on the face, affecting people between 17 and 79 years old (mean = 47 years old). Its etiology is still unknown.2 Cutaneous ossification can be classified as primary when bone tissue develops in the skin and is observed early after birth or during childhood, with the absence of preexisting skin lesions or calcium and phosphorus metabolic abnormalities. This condition may possibly be associated with Albright's hereditary osteodystrophy, fibrodysplasia ossificans progressiva, progressive osseous heteroplasia and Gardner's syndrome. It may also arise in isolation, with no association to other diseases, manifesting as a single small osteoma, a single large plate-like osteoma, multiple disseminated osteomas, or multiple miliary osteomas on the face.1,4-6 Secondary cutaneous osteomais more common, accounting for 70-85% of cases and occurring when bone tissue develops in preexisting skin lesions. Secondary cutaneous osteomascan be of neoplastic origin (such as melanocytic nevi, pilomatricoma and basal cell carcinoma) or inflammatory origin (such as scleroderma, systemic erythematosus lupus and dermatomyositis). It can also appear on post-operative scarring,or following folliculitis, chronic venous insufficiency, calcinosis,or trauma.1,5 Multiple idiopathic osteomas are most commonly reported on the faces of women with no history of acne. Nonetheless, the precisecorrelation between cutaneous osteoma and acne remains unclear.7
A 47-year-old female patient came to a medical appointment complaining of facial darkening (which had been taking place for about 24 months), and a history of untreated acne (since the age of 16).
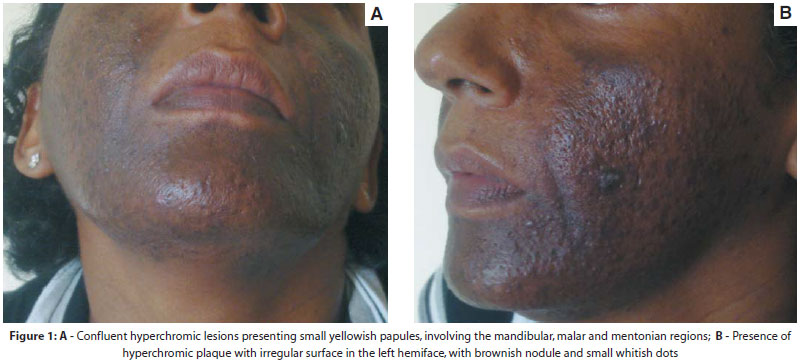
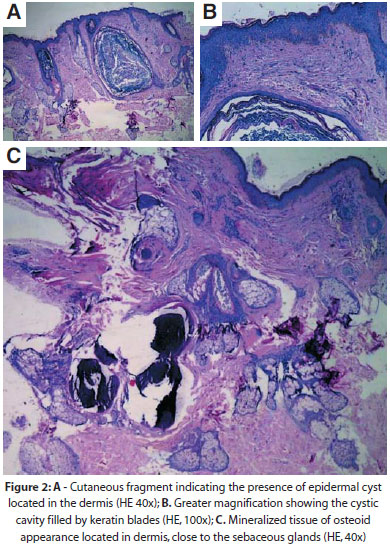
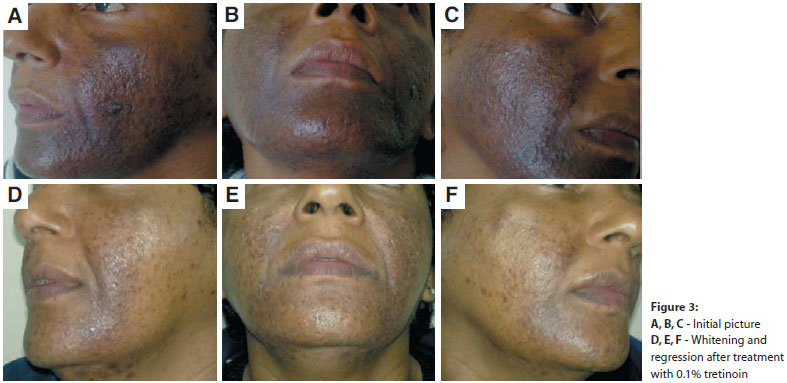
Dermatological examination showed a hardened, poorlydefined papular plaque of dark-brown hue and an irregular surface affecting the malar and mentonian regions. The papular plaque was formed by papulonodular hyperchromic lesions, some of them of yellowish-white hue (Figure 1). Followingan incisional biopsy, histological examination revealed fragments of mineralized tissue with an osteoid characteristic located within the dermis, in addition to the presence of an epidermal cyst (Figure 2). Histopathologic diagnosis suggested an epidermal cyst associated with cutaneous osteoma. Serum levels of calcium/phosphate, alkaline phosphatase and parathyroid hormone proved unaltered.Following the initial consultation, the patient was instructed to apply 0.1% tretinoin cream. Four months later, there was significant improvement in hyperpigmentation (Figure 3).
The term osteoma cutis was originally described by Wilkins in 1858, corresponding to the presence of mature bone tissue, in the dermis and/or hypodermis. The condition is a rare, benign dermatosis, classified as primary when arising early in life in healthy skin, and secondary when associated with preexisting neoplastic or inflammatory skin lesions (representing 70-85% of cases).1,6 Secondary ossifications of the face occur almost exclusively in women with a history of long-lasting inflammatory acne, 6 as in the present case. However, the precise correlation between cutaneous osteoma and acne remains unclear.7 MCMO arise in locations that coincide with those of the onset of acne vulgaris lesions (most often on the face) and when there is ahistory of this condition (55% of cases). It has been suggested that osteomas are secondary to dystrophic alterations in acne scars. The role of estrogen has been discussed, however it does not seem to be crucial in the formation of osteoma, since postmenopausal women, and some men also develop such lesions. 2 Several MCMO cases have been reported in patients without a history of acne or other inflammatory conditions, such as that of a 75-year-old female patient with an incidental histological finding of exogenous ochronosis, resulting from the use of hidroquinone. 3,7
In the present case, the patient sought medical care due to hyperchromia in the affected areas. No confirmation was available as to whether she had previously used any medication to treat acne, or used skin lighteners containing hydroquinone.
The main histological features are multiple bone spicules of varying shapes and sizes in the dermis, extending as far as the subcutaneous tissue. Such bone spicules contain numerous osteocytes, as well as cement lines. Havers ducts containing blood vessels and connective tissue can be observed in some areas. Osteoblasts with elongated nuclei can be seen along the margin of some osseous spicules. Some osteoclasts with multiple hyperchromatic and elongated nuclei can be found in the so-called Howship lacunae, while some osseous spicules also contain mature adipocytes aggregates.1,8
The pathogenesis of cutaneous ossification remains uncertain. It has been suggested that chronic inflammation leads to the development of small calcifications and metaplastic ossification. Stimulation of mesenchymal cells by different factors may induce their differentiation into osteoblastic cells, resulting in bone formation. While it can occur in isolation, the presence of ossification should be seen as a possible indication of the presence of associated diseases, including fibrodysplasia ossificans progressiva (McCune-Albright syndrome), hereditary osteodystrophy, progressive osseous heteroplasia and Gardner's syndrome. In this case report there was no evidence of clinical, metabolic characteristics or endocrine abnormalities corresponding to those conditions, with only a history of acne being confirmed.
Facial MCMO treatment methods are limited. The surgical technique involving incision and curettage of bone fragment, followed by suture, has been shown to be less invasive, and provides excellent results. The technique of extirpation of bone fragments after needle microincisions, followedby primary closure, is straightforward, effective, and cost effective.6 Dermabrasion or CO2 laser or Erbium:YAG lasers are mentioned as epidermis ablation processes.9 The topical application of tretinoin may in some cases have a favorable effect by promoting the transepidermal elimination of osteomas.6 The patient studied responded satisfactorily to use of 0.1% tretinoin, in daily and nightly applications, which proved to be an efficient, safe and non-invasive method for treating MCMO. The potential development of osteoma cutis should be considered in all patients with chronic inflammatory acne, because the identification of the first condition plays an important role in the treatment of the MCMO.
1. Haro R, Revelles JM, Angulo J, Fariña MC, Martın L, Requena L. Plaquelike osteoma cutis with transepidermal elimination. J Cutan Pathol. 2009; 36(5): 591-3.
2. Myllylä RM, Haapasaari KM, Palatsi R, Germain-Lee EL, Hägg PM, Ignatius J, et al. Multiple miliary osteoma cutis is a distinct disease entity: four case reports and review of the literature. Br J Dermatol. 2011;164(3):544-52.
3. Bowman PH, Lesher JL J. Primary multiple miliary osteoma cutis and exogenous ochronosis. Cutis. 2001;68(2):103-6.
4. Sethuraman G, Malhotra AK, Khaitan BK, Kumar R, Sharma VK, Kabra M, et al. Osteoma cutis in pseudohypoparathyroidism. Clin Exp Dermatol. 2006;31(2):225-7.
5. Samaniego-González E, Crspo-Erchiga A, Gómez-Moyano E, Boz-González JD, Sanz-Trelles A. Perforans multiple osteoma cutis on the leg in a young woman. J Cutan Pathol. 2009;36(4):497-8.
6. Thielen AM, Stucki L, Bran RL, Masouyé I, Germanier L, Harms M, Salomon D, Borradori L. Multiple cutaneous osteomas of the face associated with chronic inflammatory acne. JEADV. 2006;20:321-6.
7. Gfesser M, Worret W, Hein R, Ring J. Multiple primary miliary osteoma cutis. Arch Dermatol. 1998;134(5):641-3.
8. Neto TH, Nogueira Neto JCP,Prada AA, Cintra ML, Lima RB, Rached B. Osteoma cutâneo. An Bras Dermatol.1995; 70(1): 39-41.
9. Duarte IGL. Lesões múltiplas de osteoma cutis na face: terapêutica minimamente invasiva em pacientes com sequela de acne - Relato de casos. An Bras Dermatol. 2010;85(5):695-8.
This study was carried out at the Dermatology Service of the Universidade Federal de Uberlândia (UFU) – Uberlândia (MG), Brazil.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}