


Alceu Luiz Camargo Villela Berbert1; Adriano Mota Loyola2; Sônia Antunes de Oliveira Mantese3; Bruno César Dornela4; Mabel Duarte Alves Gomides5
Neurofibromatosis type 1, also known as von Recklinghausen neurofibromatosis, is an autosomal dominant disorder that affects 1 in 3,000 newborns. Approximately 50% of neurofibromatosis type 1 patients have no family history of the disease. The tongue, the alveolar ridge of the buccal mucosa, gums, lips, palate, floor of the mouth, and pharyngomaxillary fossa can be affected by tumors associated with this condition; the tongue is the most common site. We report the case of a 29-year-old female patient with neurofibroma in the tongue, highlighting the possibility of disease manifestations in the oral cavity and differential diagnoses.
Keywords: NEUROFIBROMATOSIS 1; NEUROFIBROMA, PLEXIFORM; NEUROFIBROMA; TONGUE NEOPLASMS.
Neurofibromatosis type 1 (NF1), also known as von Recklinghausen neurofibromatosis, is a dominant autosomal disease that affects 1 in 3,000 newborns. Approximately 50% of NF1 patients have no family history of the disease, 1 which is clinically characterized by the presence of café-au-lait spots, axillary ephelides, Lisch nodules, and multiple neurofibromas. It can be associated with optic gliomas, neurofibromas in peripheral and spinal nerves, neurological or cognitive deficit, scoliosis, oral and maxillofacial abnormalities, malignant nerve sheath tumors, pheochromocytoma, and vasculopathy.1-4
A clinical radiological study has detected soft tissue oral manifestations in 72-92% of NF1 patients, including intraoral tumors in approximately 25% of cases. The tongue, alveolar ridge of the buccal mucosa, gums, lips, palate, floor of the mouth and pharyngeal maxillary space can be affected by tumors in association with NF1, with the tongue being the most common site. 1,3,5
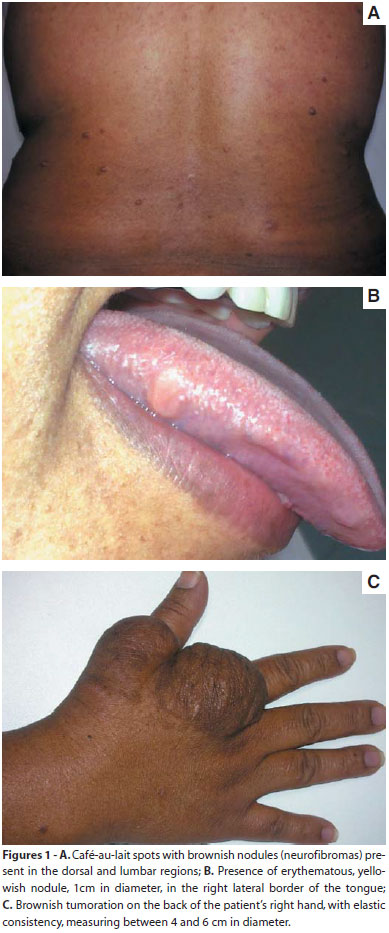
A 29-year-old female patient, born in the city of Imperatriz (in the northeast Brazilian state of Maranhão) but then living in the city of Araguari (in the Brazilian state of Minas Gerais), with grayish-brown skin, sought care at the Dermatology Service of the Universidade Federal de Uberlândia (MG), Brazil, complaining of unsightly skin lesions that had emerged in childhood and had grown gradually. The patient reported a previous diagnosis of neurofibromatosis, having denied any family history of the disease. Dermatological examination showed papulonodular and soft tumors with a hernial ring perceptible to the touch, slightly brownish in color, and located in different areas of the skin; caféau-lait macules located in the trunk and limbs; and the presence of axillary ephelides. Intraoral examination also evidenced an erythematous, yellowish, soft, painless nodular lesion, roughly 1cm in diameter, and located on the right lateral border of the tongue (Figures 1A, B and C).
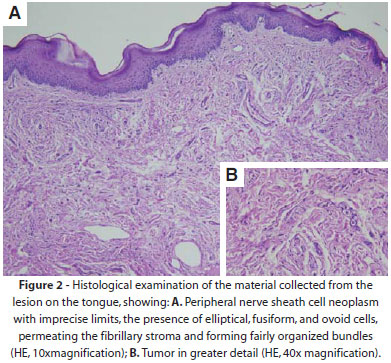
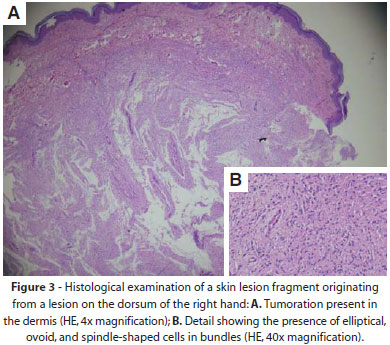
The histology of the oral lesion suggested mesenchymal nature, lined by stratified squamous epithelium, with focal areas of hyperparakeratosis, spongiosis and hydropic degeneration. Specific examination of the sections evidenced interwoven bundles of cells with elongated nuclei, distributed around nerve bundles and slightly fibrillar conjuctive tissue, with focal areas of myxoid material (Figure 2). A similar situation was found in the material collected from the lesion located on the right hand (Figure 3).
Given the clinical and histologic features presented by the patient, the diagnosis of neurofibroma was established.
NF1 is a dominant autosomal genodermatosis associated with deletions, insertions or mutations of the tumor suppressor gene NF1, located in the pericentromeric region of the chromosome 17. In general, NF1 is clinically diagnosed based on the cutaneous manifestations and family history.1 Oral alterations of NF1 were reported to vary from four to 92% of cases, with the tongue being the most common site.3,4,6
The considerable difference in oral manifestations can be attributed to the heterogeneity of the patients examined at specialized hospitals, and to differences in the investigated symptoms and research methods.1 Early diagnosis of asymptomatic neurofibromas in the tongue requires a high index of clinical suspicion. Symptomatic oral lesions are more easily diagnosed when the tumor exerts compression or other types of discomfort. A significant positive correlation was found between the delay in the diagnosis and the oral location of lesions. The presence of discomfort is reported by most patients with lesions on the tongue, with pain being the most common complaint.1 Lesions located on the tongue develop slowly. Nevertheless, tumor growth can be accelerated by puberty, pregnancy and growth, with the clinical and histological findings being key to distinguishing between neurofibromas and other soft tissue tumors.
The differential diagnosis of tumors located in the tongue includes plexiform neurofibroma, lipoma, angiolipoma, chondroid lipoma, myolipoma, hamartoma, schwannoma, lymphangioma, granular cell tumor, leiomyoma, hemangioma, rhabdomyosarcoma, neurofibroma and localized amyloidosis.1,5,6
A thorough histological analysis, assisted by the use of immunohistochemistry is essential for the correct diagnosis of soft mouth tumors. S100 protein, type IV collagen and the molecule CD34 are useful biomarkers in the analysis of NF1 with oral manifestations.1
Partial or total surgical exeresis of tumors can be carried out to resolve aesthetic and functional problems. However, waiting for the end of a tumor’s growth cycle is recommended in order to reduce the risk of recurrence, always keeping in mind the possibility of malignant degeneration (occurring in one to 29% of cases) with the appearance of peripheral nerve sheath malignant tumors.1
Such tumors are not radiosensitive and, given their slow growth rate, limited benefit has been seen with the use of chemotherapy. Alternatives to surgical treatment of plexiform neuromas are still largely experimental, but include: retinoic acid, ketotifen fumarate, antiangiogenic drugs (alpha-interferon), thalidomide, pirfenidone (drugs with antifibrotic action) and tipifarnib (a farnesyl transferase inhibitor, since high levels of that enzyme are found in plexiform neuromas). Nonetheless, evidence of the efficacy of each of these treatments remains limited. Additional research with pharmaceutical alternatives should improve survival rates and quality of life for patients with plexiform neuromas.6
Searching for oral lesions in patients with NF1 is of paramount importance, and given that the examination of mucous membranes is increasingly relevant in the daily routine of dermatologists, it provides new tools for the elaboration of diagnostics. It is therefore necessary that the specialist dermatologist be familiarized with the different types of lesions that may be found in the various genodermatoses.
1. Bongiorno MR, Pistone G, Aricò M. Manifestations of the tongue in Neurofibromatosis type 1. Oral Dis. 2006;12(2):125-9.
2. Obermoser G, Zelder BG, Millonig G, Sepp N, Vogel W, Zelger B. Vasculopathy in von Recklinghausen's neurofibromatosis-a diagnostic quandary. J Am Acad Dermatol. 2004;50(5 suppl):S107-9.
3. Jouhilahti B, Visnapuu V, Soukka T, Aho H, Peltonen S, Happonen R, et al. Oral soft tissue alterations in patients with neurofibromatosis. Clin Oral Investig. 2012;16(2):551-8.
4. Friedrich RE, Manfred Giese M, Schmelzle R, Mautner V, Scheuer HA. Jaw malformations plus displacement and numerical aberrations of teeth in neurofibromatosis type 1: a descriptive analysis of 48 patients based on panoramic radiographs and oral findings. J Craniomaxillofac Surg. 2003;31(1):1-9.
5. Nascimento GJF, Rocha DAPR, Galvão HC, Costa ALL, Souza LB. A 38-year review of oral schwannomas and neurofibromas in a Brazilian population: clinical, histopathological and immunohistochemical study. Clin Oral Invest. 2011;15(3):329-35.
6. Fabriz G, Pagliarello C, Massi G. Unusual localization of a plexiform neurofibroma in a child with neurofibromatosis 1. Clin Exp Dermatol. 2008;33(6):811-2.
This study was carried out at the Dermatology Department, Universidade Federal de Uberlândia (UFU) - Uberlandia (MG), Brazil.
 All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773
All content the journal, except where identified, under the Creative Commons Attribution 4.0 International licence - ISSN-e 1984-8773



 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket
{kind=link}
{kind=link}
{kind=link}